Download
1 / 69
700 likes | 947 Vues
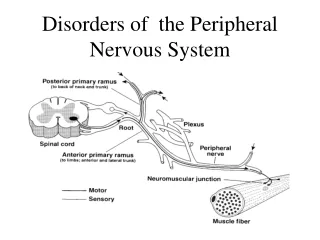
Disorders of the Peripheral Vascular System. Arterial (Non-Cardiac) and Venous. Objectives . Describe peripheral vascular disorders Name 8 common peripheral vascular disorders Explain the pathophysiology of peripheral vascular disorders.

E N D
Disorders of the Peripheral Vascular System Arterial (Non-Cardiac) and Venous
Objectives • Describe peripheral vascular disorders • Name 8 common peripheral vascular disorders • Explain the pathophysiology of peripheral vascular disorders. • Describe nursing interventions in caring for clients with peripheral vascular disorders.
Assessment of Arterial and Venous Circulation • Pulse – may be decreased r/t poor blood flow • Appearance – may be discolored, shiny, scaly • Temperature – may be cool or abnormally warm • Capillary refill – poor blood flow = >3sec • Hardness – hard = chronic stasis, risk of ulceration • Edema – pitting may indicate acute edema • Sensation – pain or numbness and tingling
Arterial Diseases (Non-Cardiac) Peripheral Arterial Disease
PAD Risk Factors • P.A.D. is caused by the build-up of fatty deposits (plaque) and cholesterol in the arteries outside the heart.
The First Tool to Establish the PAD Diagnosis:A Standardized Physical Examination Pulse intensity should be assessed and should be recorded numerically as follows: • 0, absent • 1, diminished • 2, normal • 3, bounding • 4, Cannot be obliterated Use of a standard examination should facilitate clinical communication
Ankle Brachial Index • A technique in which a hand held doppler is used to measure the ratio of ankle systolic BP to the highest brachial blood pressure • Normal = 0.91-1.30 • Mild PAD = 0.71-0.90 • Moderate PAD = 0.41-0.70 • Severe PAD = < 0.40
ABI Procedure http://www.nhlbi.nih.gov/health/dci/Diseases/pad/pad_diagnosis.html
Right ABI 80/160=0.50 Left ABI 120/160=0.75 aABA Highest brachial SBP Brachial SBP 160 mm Hg Brachial SBP 150 mm Hg PT SBP 120 mm Hg PT SBP 40 mm Hg Highest of PT or DP SBP DP SBP 80 mm Hg DP SBP 80 mm Hg Using the ABI: An ExampleNormal = >0.90 ABI=ankle-brachial index; DP=dorsalis pedis;PT=posterior tibial; SBP=systolic blood pressure.
Interpreting the Ankle-Brachial Index Adapted from Hirsch AT, et al. J Am Coll Cardiol. 2006;47:e1-e192. Figure 6.
Exercise ABI Testing: Treadmill • Indicated when the ABI is normal or borderline but symptoms are consistent with claudication*. • If the ABI results fall post-exercise - supports a PAD diagnosis; • May “unmask” PAD, if resting ABI is normal. *Claudication = tissue ischemia .
Magnetic Resonance Angiography (MRA) • MRA has virtually replaced contrast arteriography for PAD diagnosis • Excellent arterial picture
Computed Tomographic Angiography (CTA) • Requires iodinated contrast • Requires ionizing radiation • Produces an excellent arterial picture
Symptoms of Peripheral Artery Disease • Terms: • Claudication: the process of activity ischemia LE pain in affected extremity; usually subsides with rest • Intermittent Claudication = a weakness of the legs accompanied by cramping pains in the calves caused by poor circulation of blood muscles.
Symptoms of Peripheral Artery Disease Asymptomatic:Without obvious symptomatic complaint (but usually has an ABI of <.90) Classic claudication: Lower extremity symptoms confined to the muscles with a consistent (reproducible) onset with exercise and relief with rest “Atypical” leg pain: Lower extremity discomfort (foot, toe, or leg pain) that is exertional but that does not consistently resolve with rest
Signs and Symptoms of Peripheral Artery Disease Critical limb lschemia:Pain at rest, non-healing wound (8-12 weeks), or gangrene Acute limb ischemia (Arteriosclerosis Obliterans):The five “P”s, defined by the clinical symptoms and signs that suggest potential limb jeopardy: • Pain • Pulselessness • Pallor • Paresthesias • Paralysis • (& polar sensation (coldness), as a sixth “P”).
Options in Limb Revascularization • Endovascular reconstruction options • Percutaneous transluminal angioplasty (PTA) • Stents • Surgical reconstruction options • Endarterectomy • Embolectomy • Aortoiliac/aortofemoral reconstruction • Femoropopliteal bypass (above knee and below knee) • Femorotibial bypass
Critical Limb Ischemia – Nursing Interventions • Assessment: 5- P’s • Maximize tissue perfusion • Treat pain • Reduce risk factors • Positioning • Reposition at least every 2 hours • Avoid crossing legs • Legs in dependent position if tolerated by patient • Keep linens off extremity by using foot cradle • Avoidance of vasoconstrictors • ETOH, nicotine, stress, cold
Post-op Surgical Revascularization: Nurse Management • Monitor VS • Assess 5 P’s • Check peripheral pulses (doppler) frequently • Check operative site for bleeding or infection • Measure abdomen for increasing size • If symptoms of bleeding or rupture occurs, immediate intervention needed
Thromboangiitis Obliterans(Buerger’s Disease) • Disorder of unknown cause where the small and medium-sized arteries become inflamed and thrombotic • Affects primarily the feet and hands Strong correlation with smoking: The classic Buerger’s Disease patient is a young male (e.g., 20–40 years old) who is a heavy cigarette smoker. • Confirmed by angiogram
Signs and Symptoms of Beurger’s Disease • Extremely painful, especially in non-diabetics with normal sensation • Claudication: Pain induced by insufficient blood flow during exercise • Most common in the Orient, Southeast Asia, India and the Middle East • Decreased perfusion • Cold, pale, skin • Ulcers, necrosis of skin • Sensitivity to cold
Medical Management • Focus is on preventing progression of the disease by modifying risk factors • In many cases quitting smoking will cure the disease • Surgical intervention may be necessary in cases of advanced necrosis • Surgical interruption of nerve pathways may be performed (rarely) in cases involving extreme pain
Raynaud’s Disease • Intermittent arterial spasms causing ischemia to the periphery • Usually precipitated by cold or emotional stimuli • Cause is unknown • May be associated with other autoimmune conditions
Signs and Symptoms of Raynaud’s Disease • Chronically cold hands and feet • Pallor • Numbness • Cyanosis of nailbeds • Pain
Medical Management • Diagnosed by cold stimulation test • Skin temperature changes are recorded after submersion in ice bath • Submerge patient’s hand in an ice water bath for 20 seconds and record ongoing temperatures • Skin temperature changes are recorded by a thermistor attached to each finger
Medical Management • Medications used to treat • Calcium channel blockers • Relax smooth muscles of the arterioles • Relaxation and stress management • For extreme pain, surgical intervention may interrupt nerve pathways
Raynaud’s Patient Teaching • Avoid temperature extremes • Avoid vasoconstricting agents • Wear mittens/gloves and warm socks for any exposure to cold • Weather • Fridge/freezer or frozen foods
Arterial Aneurysm • True Aneurysm • Focal dilation within an artery. • Differentiated from pseudoaneurysm because the dilated area of the vessel contains all three layers. • Common Etiologies: • Atherosclerosis • Congenital or genetic predisposition (Marfan’s) • Trauma to vessel wall (usually causes pseudoaneurysm)
Arterial Aneurysm • Marfan Syndrome • A connective tissue multisytemic disorder • Characterized by skeletal changes, long limbs, joint laxity, cardiovascular defects (aortic aneurysm, mitral valve prolapse), mutation in the fibrin-1 gene.
Arterial Aneurysm • Risk (higher with smoking and hypertension) • Rupture • Dissection • Thromboembolism • Common Locations • Abdominal Aorta • Ascending Aorta (Aortopathy, also associated with bicuspid aortic valve) • Popliteal • Cerebral Aneurysms (increased risk of SAH)
Types of Arterial Aneurysms • Fusiform • Saccular • Dissecting or Pseudo- aneurysm
Arterial Aneurysm • Signs and Symptoms • Dependent on location of aneurysm • Pulsating mass may be felt in superficial arteries • Symptoms may be due to: • Local mass effect/compression of other structures • Hoarsness, low urine output, GERD • Rupture • Low BP, Pain • Thromboembolism
Aneurysm Rupture • Aortic aneurysm ruptures present with severe chest, back, or abdominal pain (depending on location) and are often fatal • Cerebral aneurysm ruptures present with “worst headache of life” and subarachnoid hemorrhage (SAH). Also may have stroke symptoms
Medical Management • Control of HTN is essential to reduce the risk of rupture • Beta blockers are especially preferred due to slowing of heart rate and the rate of rise of blood pressure • Surgical intervention to repair aneurysm varies depending on type and location of aneurysm
Nursing Care • Nursing management of pre-operative aneurysm pt. focuses on controlling HTN (with medication) and monitoring for s/s of rupture • Pallor, weakness, tachycardia, hypotension, sudden onset abdominal, chest, back or groin pain; abd. pulsating mass • Post-operative management focuses on maintaining effective tissue perfusion • Teaching includes prevention and management of atherosclerosis and HTN • Risk Factor Reduction
Venous Insufficiency • Blood regurgitates through the valves in the veins and then “leaks” into the tissue, causing edema • Chronic venous insufficiency can cause an area of the skin to turn darker and become dry and scaly • Eventually chronic edema (stretching) can lead to ulcerations of the skin Normal Blood Flow
Venous Stasis Venous Stasis Ulcer
Venous Stasis Ulcers • Occur from chronic deep vein insufficiency and, • Stasis of blood in the venous system of the legs • A leg ulcer = an open, necrotic lesion • Results when an inadequate supply of oxygen-rich blood and nutrients reaches the tissue cell death, tissue sloughing, and skin impairment
Venous Stasis Ulcers • Signs and Symptoms: • Most significant sign is the ulceration • Skin will be darkened around ulcerated area • Varying degrees of pain • If diabetic, may not have any pain • Edema • Pedal pulses often present
Venous Stasis Ulcers • Medical Management • Focus on wound healing • The wound will not heal if the skin continues to be stretched • Use TED hose or ACE wrap and elevate the legs whenever possible • Treatment of infection if needed • Nutrition with adequate protein
Venous Stasis Ulcers • Medical Management cont. • Debridement of necrotic tissue if needed • Unna’s paste boot • Protective boot that can be left on for 1-2 weeks • (next slide)
Unna’s Boot is a medicated bandage that provides gradient compression therapy for controlling venous ulcers, venous insufficiencies, and other minor orthopedic problems. The bandage is permeated with zinc oxide and calamine to comfort the skin. Unna’s Boot is commonly used for active patients who are not confined to a wheelchair or bed. Unna’s Boot comes in the form of a non-raveling gauze that will mold evenly to the applied limb. Once applied, the bandage forms a semi-rigid cast that provides high working pressure and a lower resting pressure. This is ideal for patients who actively walk around and would like to preform normal daily activities. The 100% cotton base reduces wastage and the calamine prevents skin irritation. Depending on the amount of drainage from the ulcer, Unna’s Boot is usually kept in place for 3-7 days. A self-adherent wrap can also be wrapped around Unna’s Boot for extra support.
Varicose Veins • Tortuous dilated vein with incompetent valves • Usually in lower extremities • Higher incidence in women aged 40-60 • Risk: family tendency, congenital abnormalities, pregnancy, obesity, constrictive clothing, and prolonged standing
Varicose Veins • Pathophysiology • Incompetent valves Veins lose elasticity • Relatively weak vessel walls (compared to arteries) Unable to support the increased pressure of the blood within the vessel Vein dilates as blood in it flows backward
Varicose Veins • Signs and Symptoms: • Vary according to area of varicosity • May appear as darkened areas on the surface of the skin • May experience dull aches, fatigue, cramping, heaviness of legs • May shows sign of venous stasis