Download
1 / 1
50 likes | 469 Vues
Leiomyosarcoma of the Inferior Vena Cava: Case Report and Review of Literature. Jennifer R. López López 1 , Gloriel Flores Cabán 1 , Juan Luis Pérez Berenger 1,2 , Luis Ferrer Torres 2 , Luis Aponte López 3 , José Valderrabano 4

E N D
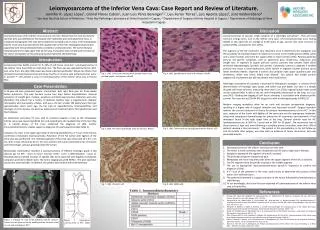
Leiomyosarcoma of the Inferior Vena Cava: Case Report and Review of Literature. Jennifer R. López López1, Gloriel Flores Cabán1, Juan Luis Pérez Berenger1,2, Luis Ferrer Torres2, Luis Aponte López3, José Valderrabano4 1 San Juan Bautista School of Medicine, 2Hato Rey Pathology Laboratory at Hima Hospital in Caguas, 3 Department of Surgery at Hima Hospital in Caguas, 4 Department of Radiology at Hima Hospital in Caguas Abstract Discussion Leiomyosarcomas of the inferior vena cava are very rare. We present the case of a 54 year old man who was admitted to the hospital with right flank pain and abdominal mass. A computed tomographic (CT) scan of the abdomen revealed a 10 cm mass in the infrahepatic inferior vena cava that extended to the caudate lobe of the liver. Histological examination supported with immunohistochemistry revealed a Leiomyosarcoma. The tumor had also metastasized to the right upper lobe of the lung. The patient was treated with resection of the tumor and ligation of IVC, followed by post-operative chemotherapy. Leiomyosarcomas of vascular origin comprise of a seemingly rare group1. They are most common in large veins, such as the inferior vena cava1. IVC leiomyosarcomas occur during middle or late adult life, on average at 52.65 years of age, and are also most common in women (78%), compared to men (22%). The segment of the IVC involved is very important since it determines the symptoms and the possibility of resection (Figure 2). Most tumors arise in the middle portion (60%), while only a small number arise from the upper (15%) or lower portion (25%). Patients generally present non-specific symptoms, such as abdominal pain, tenderness, exhaustion and weight loss. In segment III (upper portion) tumors, patients may present Budd Chiari syndrome (hepatomegaly, jaundice and ascites). Conversely, tumors in segment II (middle portion) may result in renal dysfunction, while tumors in segment I (lower portion) cause lower extremity edema. Segment II tumors also produce right upper quadrant pain and tenderness, which may mimic biliary tract disease1. Our patient had middle portion (segment II) involvement but did not present renal dysfunction. Pathologic assessmentof sarcomas is essential for therapeutic strategies. It consists of the determination of histologic type, grade, and tumor size and depth. Our case is a deeply situated soft tissue sarcoma, measuring more than 5 cm (T2b), regional lymph nodes could not be assessed (NX). A LMS of the IVC more frequently metastasize to the lung, as in our case (M1). Grading and staging of soft tissue sarcomas is associated with disease-specific survival. Our case was a pT2b NX M1 (stage four) with a histological grade 2 (FNCLCC). Modern imaging modalities allow for an early and accurate preoperative diagnosis, resulting in a higher rate of surgical resection and improved survival4. Surgical resection remains the current treatment of choice for primary leiomyosarcomas of the IVC3. In this case, resection of the tumor with ligation of the vena cava was the appropriate treatment, along with subsequent chemotherapy for prevention of recurrence and treatment of the metastasis found in the right upper lobe of the lung. General survival rates for IVC leiomyosarcomasare at 50% for 5 years and at 30% for 10 years6. The recurrence rate of these tumors is high and, even following a complete primary resection, more than 50% of patients develop a late recurrence7. The patient in this presentation, in his last follow-up visit 20 months after surgery, was alive with no evidence of tumor recurrence, and only presented anemia. Introduction Leiomyosarcomas (LMS) account for 5–10% of soft tissue sarcomas1. Leiomyosarcomas of the Inferior Vena Cava (IVC) are extremely rare. The first case was reported by Perl on 1871 and, since then, less than 300 cases have been reported worldwide2. About two thirds of all retroperitoneal leiomyosarcomas and three fourths of all vena cava leimyosarcomas occur in women1,3,4. We present acase of a leimyosarcoma of the inferior vena cava in Puerto Rico. Fig. 3. LMS. Soft tissue sarcoma with spindle tumor cells, marked atypia, and mitoses. HEx40 Fig. 4. LMS. Spindle tumor cells with mitoses. HEx40 Case Presentation A 54-year-old man presented severe, intermittent, dull, right flank pain for three weeks before admission. The pain became severe four days before hospitalization. General symptoms of weight gain, malaise, weakness and decreased exercise tolerance were also identified. The patient has a history of diabetes mellitus type 2, hypertension, diabetic retinopathy and neuropathy, strokes, and was a chronic smoker (30 packs/year) that quit approximately seven years ago. He has had an appendectomy, cholecystectomy and drainage of a toe abscess. He also has paternal and maternal history for hypertension and heart disease. An abdominal and pelvic CT scan with IV contrast revealed a mass at the infrahepatic inferior vena cava, measuring 80.82 mm and extending to the caudate lobe of the liver (Fig. 1). A needle biopsy of the mass confirmed the diagnosis of LMS. Further immunohistochemistry studies support a diagnosis of Leiomyosarcoma (See Table 1). A biopsy of a mass in the right upper lobe of the lung identified by a CT scan of the thorax, confirmed a metastatic leiomyosarcoma. Resection of the IVC tumor with ligation of the vena cava was performed. The resected segment of the vena cava measured 10 x 6.5 x 4.5 cm, with a mass measuring 10 cm. On cross section, the tumor presented areas of necrosis and hemorrhage, and was growing inside the lumen. Microscopic examination revealed a Leiomyosarcoma of FNCLCC histologic grade 2 (24 mitoses per 10 HPF - score 3; tumor necrosis <50% - score 1; differentiation - score 1). Perpendicularly oriented fascicles of spindle cells were observed with brightly eosinophilic cytoplasm and blunt-ended nuclei. The tumor staging was pT2b NX M1 . The post-operative course was unremarkable. In addition, the patient was treated with chemotherapy. Fig. 6. LMS. Tumor cells are strongly positive for desmin. x20 Fig. 5. LMS. The tumor presented areas of necrosis. HEx10 Conclusion • Leiomyosarcomasof the inferior vena cava are very rare. • The tumor is most commonly seen in patients over 50 years of age and in females. • Symptoms depend of the segment of the IVC involved. • The principal symptom is abdominalpain. • Metastases are more frequently seen when the upper segment of the IVCis involved. • The IVC segment most frequently involved is the middle segment • The use of appropriate immunohistochemistry panels is important to confirm the diagnosis of LMS. • A CT scan of the abdomen is the most useful study to determine the location of the tumor and treatment plan. • The preferred treatment is surgical resection of the tumor followed by chemotherapy or radiotherapy. • To our knowledge, this is the first case reported of Leiomyosarcoma of the inferior vena cava in Puerto Rico. Fig. 7. LMS. Vimentin x20 Fig. 8. LMS. ASMA x20 References • EnzingerFM, Weiss SW, Goldblum JR. Leiomyosarcoma. In: Abdul-Karim FW, Folpe AL, Antonescu CR, eds. Soft Tissue Tumors. 4th ed. St. Louis, MO: Mosby; 2001: 727-746. • Murguia-Pérez M, López-Zuñiga D, Cruz-Gordillo AG, León-Martínez G, Navarro-Córdoba FDJ, Mendoza-Ramírez S. Leiomiosarcoma de la vena cava inferior. Presentación de un caso y revision del cuadro clinicopatológico. Rev Esp Patol. 2011; 44 (2): 132-135. • Alexander A, Rehders A, Raffel A, Poremba C, Knoefel WT, Eisenberger CF. Leiomyosarcoma of the inferior vena cava: Radical Surgery and vascular reconstruction. World Journal of Surgical Oncology. 2009; 7: 56. • Reddy VP, VanVeldhuizen PJ, Muehlebach GF, et al. Leiomyosarcoma of the inferior vena cava: a case report and review of the literature. Cases Journal. 2010; 3: 71. • Abisi S, Morris-Stiff GJ, Scott-Coombes D, Williams IM, Douglas-Jones AG, Puntis MC. Leiomyosarcoma of the inferior vena cava: Clinical experience with four cases. World Journal of Surgical Oncology. 2006; 4: 1. • Fisher C, Mentzel T, Thway K, et al. Leiomyosarcoma. In: Montgomery EA, Lucas DR, Srivastava A, eds. Diagnostic Pathology: Soft Tissue Tumors. 1st ed. Canada: Amirsys; 2011: 22-29. • Shvarts O, Han KR, Lam JS, Belldegrun AS. Primary Leiomyosarcoma of the Inferior Vena Cava Presenting as a Renal Mass. Reviews in Urology. 2004; 6 (1): 39-42. Figure 1: Coronal CT scan of the abdomen with IV contrast. A mass can be observed in the middle portion, between renal vessels and retrohepatic IVC. Figure 2: Anatomical classification of IVC LMS 5.