Download
1 / 101
1.09k likes | 1.74k Vues
Chapter 8 Diagnostic Enzymology And Other Biochemical Markers Of Organ Damage. Lixia Zhang. Contents. Basic Concepts For Diagonostic Enzymology Enzyme Assay Procedures Liver Diseases * Markers Of Liver Diseases

E N D
Chapter 8Diagnostic Enzymology And Other BiochemicalMarkers Of Organ Damage Lixia Zhang
Contents Basic Concepts For Diagonostic Enzymology Enzyme Assay Procedures Liver Diseases * Markers Of Liver Diseases * Patterns Of Liver Enzymes And Markers For Interpretation Of Disease * Myocardial And Skeletal Muscle Disease * Pancreatic Diseases Miscellaneous Enzymes Suggested Readings * Important
●Diagnostic enzymology involves the measurement of enzymes in body fluids for the diagnosis of disease. In most cases, serum or blood levels are the most useful, although urine, cerebrospinal, and extracellular fluid levels are sometimes important. ● This chapter focuses on the analytical aspects and clinical significance of important enzymes that are measured for diagnostic purposes.
● The major emphasis is on the use of these enzymes for the diagnosis of diseases involving the liver, myocardium, skeletal muscle, pancreas, and bone. In the case of myocardial infarction and skeletal muscle injury, nonenzyme markers such as myoglobin and troponin are also discussed.
Pathologic Role of Enzymes in Blood -1 ●Most enzymes that are used for diagnostic purposes have no direct physiologic role in the blood: Their presence under normal circumstances is the result of natural aging and turnoverof cells.
Pathologic Role of Enzymes in Blood -2 ●The normal level of activity of these enzymes in the serum is a function of the rate of release and clearance. ● The half-lives of these enzymes vary greatly from an estimated 2 hours for the BB isoenzyme of creatine kinase (CK) to 170 hours for placental alkaline phosphatase (ALP).
Pathologic Role of Enzymes in Blood -3 ●High levels of enzymes in the blood can indicate increased cellular turnover and tissue necrosis caused by disease. ● An equally important and largely overlooked cause of high enzyme levels in blood is tissue synthesis of new enzymes that occurs in response to disease, induction by various drugs, and carcinogenesis.
ENZYME ASSAY PROCEDURES ●Single-Reagent Kinetic Assays ● Start Reagent Activity Assays ● Enzyme Activity Calculations ● Mass Measurements
Mass Measurements ●These assays are particularly useful for isoenzyme analysis, as antisera can be directed toward specific isoenzymes, isoforms, or subunits. ●Mass measurements are also used to measure the concentration of protein markers (e.g., myoglobin) that do not possess enzymatic activities.
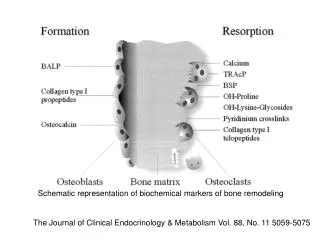
LIVER ANATOMY LIVER
LIVER DISEASES ● The enzymes ALT and AST, ALP, LDH, GGT, and (to a lesser extent) 5'-nucleotidase (5'NT) are commonly measured for the assessment of liver function. ● None of these markers is specific for any single liver disorder.
LIVER DISEASES ●This section covers liver dysfunction, describes individual liver enzymes and their laboratory measurement , and explains how patterns of liver enzyme data can be used to aid in the diagnosis of liver diseases.
LIVER DISEASES Inclusion: ● Acute Hepatocellular Injury ● Cholestatic Liver Diseases ● Chronic Liver Diseases ● Alcoholic Liver Disease
Specific enzymes of liver ●ALP ( Alkaline Phosphatase) and ALP Isoenzymes ● GGT ( g-glutamyl-peptide : amino acid γ- glutamyltransferase) ● 5'-NT ( 5'-ribonucleotide phosphohydrolase) ● AST ( L-aspartate : 2- oxoglutarate amino- transferase ) ● ALT (L-alanine: 2-oxoglutarate amino-transferase)
ALT 20%AST GGT 80% AST ALP
Plasma alkaline phosphatase activity as a function of age and sex(—men;……, women). Horizontal lines refer to multiples of the adult upper reference limit.
PATTERNS OF LIVER ENZYMES AND MARKERS FOR INTERPRETATION OF DISEASE
● Unlike some disorders such as acute pancreatitis and myocardial infarction, for which there are enzyme markers that are primarily used for one disorder and have high diagnostic efficiencies, there are no enzyme markers that are specific for any single liver disease.
●When evaluating these disorders, therefore, it is appropriate to consider a panel of markers, sometimes called live function tests (LFTs). ● usually includes bilirubin, AST, ALT,ALP,and sometimes GGT and 5'NT ● although these tests can reflect various disease processes in the liver, they do not reflect hepatic reserve for synthesis and metabolic functions
Acute Injury When Acute Hepatocellular Injury : ■ AST and ALT and are therefore rarely used for diagnostic purposes. ■ ALP, GGT, and 5'NT are not as markedly elevated.
Cholestasis -1 ● The best markers for intrahepatic and extrahepatic cholestasis are ALP, GGT, and 5'NT ● The largest elevations (four- to 10-fold) of ALP are typically seen in obstruction owing to gallstones or malignancy and in biliary cirrhosis.
Cholestasis -2 AST and ALT are generally only slightly elevated in cholestasis, rarely more than 500 U/L. Measurement of total and direct bilirubin are also important in making the diagnosis of obstructive jaundice.
Relationship of AST and ALT to ALP and GGT in Cholestasis Multiplies of normal
De Ritis Ratio (AST/ALT)-1 Further differentiation of specific liver diseases is aided by calculating the ratio of AST to ALT levels. — acute or chronic ? — intra- or extrahepatic ? recommended by the International Federation of Clinical Chemistry (IFCC) de Ritis ratio is normally approximately 1.15
ALT versus AST levels in various liver diseases
De Ritis(AST/ALT) -3Intrahepatic and Extrahepatic obstruction
De Ritis(AST/ALT) - 4Intrahepatic and Extrahepatic obstruction Other laboratory tests: ALP extrahepatic >intrahepatic Conjugated bilirubin extrahepatic >intrahepatic Amylase extrahepatic >intrahepatic
Relationship of AST and ALT to ALP and GGT in Malignancy Multiplies of normal