Download
1 / 143
1.48k likes | 1.81k Vues
Fluid and Electrolyte Balance during Injury. Zohair Al Aseri. MD. FCEM(UK).FRCPC (EM&CCM) Chairman ,National Emergency Medicine Committee Coordinatoor MPH-DME Master Consultant, ICU Department of Critical Care Chairman, Department of Emergency Medicine

E N D
Fluid and Electrolyte Balance during Injury Zohair Al Aseri. MD. FCEM(UK).FRCPC (EM&CCM) Chairman ,National Emergency Medicine Committee Coordinatoor MPH-DME Master Consultant, ICU Department of Critical Care Chairman, Department of Emergency Medicine College of Medicine, King Saud University Medical City. Riyadh, KSA. zalaseri@ksu.edu.sa http://fac.ksu.edu.sa/zalaseri
Fluid and Electrolyte Balance during Injury • Objectives • Understand of The Normal Regulation of Fluid Balance • Fluid Imbalance In Shock State • Early Hemodynamic Optimization • Fluid Therapy (Types) & Indication • Electrolyte disturbances in trauma and surgery • Acid base in surgery patients
Case 1 39 year old male involved in MVC brought to ED by EMT, he is unconscious, hr 120 bp 80/50, intubated in the scene, what is your immediate action • Take further history • Start him on dextrose 5% with NS • Start him in colloid • Start him in Normal saline
Case2 A recovery nurse calling you to see a 70 year old male, 7 hours post appendicictomy, because he is drowsy and unresponsive, his vital signs are normal and oxygen saturation 92% on room air? What is the most likely diagnosis? • Intracranial bleeding • Stroke • Acute renal failure • Respiratory failure
Case3 70 year old male, admitted for elective hernia repair, kept NPO and started in D5 ½ normal saline 24 hour ago, his current electrolyte showed k of 5 mmol and Na of 128 mmol What is the most likely diagnosis? • DI • SAIDH • Acute renal failure • Iatrogenic hyponatremia
Fluid and Electrolyte Balance during Injury Hypovolaemia • Reduced circulating volume Causes • Loss of blood, electrolyte-containing fluid or water. • 'third-space loss', due to increased vascular permeability.
Hypovoluemia will reduce oxygen and nutrient delivery and so increase healing and recovery times.
Fluid and Electrolyte Balance during Injury Fluid-conserving measures Oliguria and sodium and water retention • Due to the release ADH and aldosterone is common after major surgery or injury • May persist even after normal circulating volume has been restored.
Fluid and Electrolyte Balance during Injury Fluid-conserving measures: Increased ADH Secretion from the posterior pituitary is response to • Afferent nerve impulses from the site of injury • Atrialstretch receptors (responding to reduced volume)and the aortic and carotid baroreceptors (responding to reduced pressure) • Increased plasma osmolality (principally the result of an increase in sodium ions) detected by hypothalamic osmoreceptors. • Input from higher centres in the brain (responding to pain, emotion and anxiety).
Fluid and Electrolyte Balance during Injury Fluid-conserving measures: • ADH promotes the retention of free water (without electrolytes) by cells of the distal renal tubules and collecting ducts.
Fluid and Electrolyte Balance during Injury Aldosterone secretion from the adrenal cortex is increased by: • Activation of the renin-angiotensin system. • Renin is released from afferent arteriolar cells in the kidney in response to reduced blood pressure and activation of the renal sympathetic nerves.
Fluid and Electrolyte Balance during Injury Aldosterone secretion from the adrenal cortex is increased by: • Renin converts circulating angiotensinogen to angiotensin AT-1. • AT-1 is converted by angiotsion converting enzyme (ACE) in plasma and tissues (particularly the lung) to AT-2 which cause arteriolar vasoconstriction and aldosterone secretion
Fluid and Electrolyte Balance during Injury Adrenocorticotropic hormone (ACTH) • Increased by the anterior pituitary in response to hypovolaemia and hypotension via afferent nerve impulses from stretch receptors in the atria, aorta and carotid arteries. • lt is also raised by ADH. • Direct stimulation of the adrenal cortex by hyponatraemia or hyperkalaemia.
Fluid and Electrolyte Balance during Injury • Aldosterone increases the reabsorption of both sodium and water by distal renal tubular cells with the simultaneous excretion of hydrogen and potassium ions into the urine.
Fluid and Electrolyte Balance during Injury • Increased ADH and aldosterone secretion following injury usually lasts 48-72 hours during which time urine volume is reduced and osmolality increased.
Fluid and Electrolyte Balance during Injury • urinay sodium excretion decreases to 10-20mmol /24hrs (normal 50-80mmol /24 hrs) • potassium excretion increases to> 100 mmol/24 hrs (normal 50-80mmol /24 hrs).
Fluid and Electrolyte Balance during Injury Blood flow-conserving measures: Hypovolaemia • Reduces cardiac preload which leads to a fall in cardiac output. • Increased sympathetic activity results in a compensatory increase in cardiac output, peripheral vasoconstriction and a rise in blood pressure.
Fluid and Electrolyte Balance during Injury FLUID AND ELECTROLYTE BALANCE: May be altered in the surgical patient for several reasons: • ADH and aldosterone secretion as described above. • Loss from the GI tract (e.g. bowel preparation, ileus, stomas, fistulae). • Reduced oral fluid intake in the perioperative period
Fluid and Electrolyte Balance during Injury FLUID AND ELECTROLYTE BALANCE: • Insensible losses (e.g. sweating secondary to fever). • Third space losses. • Surgical drains. • Medications (e.g. diuretics). • Underlying chronic illness (e.g. cardiac failure, portal hypertension).
Fluid and Electrolyte Balance during Injury Normal water and electrolyte balance: • Water forms about 60% of total body weight in men and 55% in women. • Approximately two-thirds is intracellular, one-third extracellular. • Extracellular water is distributed between the plasma and the interstitial space
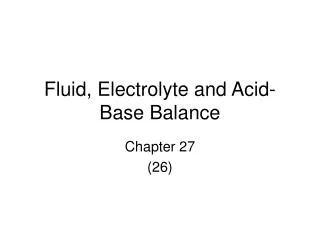
Regulation of Fluid Balance TOTAL BODY FLUID (40) liters;60%TBW The intracellular and extracellular compartments are separated by water-permeable cell membranes. Plasma volume (3 liters,5 %) Red cell volume (2 liters) Extracellular (15 liters,20%) Intracellular (25 liters,40%) Blood volume (5 liters)
IC. WATER ECF 2/3 intrest. 1/3 blood 25 150 15 0.01 2 6 50 Na K Mg Ca Cl Hco3 Phos 140 4.5 1.2 2.4 100 25 1.2 Fluid & Electrolyte Balance
Regulation of Fluid Balance ECC Osmolarity ECF Volume Maintain BP Prevent swelling or shrinking of the cells
Fluid and Electrolyte Balance during Injury Normal water and electrolyte balance: • Osmolalityof extracellular fluid (normally 275-295mOsmol /kg) determined primarily by sodium and chloride ion concentrations.
Fluid and Electrolyte Balance during Injury Normal water and electrolyte balance: • Plasma oncotic pressure is primarily determined by albumin.
Fluid and Electrolyte Balance during Injury Normal water and electrolyte balance: In adults, • Normal daily fluid requirement is 30-35ml / kg (-2500 ml /day). In newborn babies and children • Contain proportionately more water than adults. • Daily maintenance fluid requirement at birth is about 75ml/ kg, increasing to 150 ml/ kg during the first weeks of life.
Fluid and Electrolyte Balance during Injury Normal water and electrolyte balance: • After first month of life, fluid requirements decrease and the '4/2/1' formula can be used to estimate maintenance fluid requirements: • first l0 kg of body weight requires 4ml /kg/h; • the next 10kg 2ml /kg/ h; • thereafter each kg of body requires 1ml/kg/h.
Fluid and Electrolyte Balance during Injury The estimated maintenance fluid requirements of a 35 kg child would therefore be: • (10 X 4) + (10 X 2) + (15 X 1) = 75 mljh.150 . • The daily requirement for both sodium and potassium in children is about 2-3mmol/kg.
Fluid and Electrolyte Balance during Injury Assessing losses in the surgical patient:
Fluid and Electrolyte Balance during Injury Assessing losses in the surgical patient:
Fluid and Electrolyte Balance during Injury Insensible fluid losses: Hyperventilation • increases insensible water loss • is not usually large unless the normal mechanisms for humidifying inhaled air (the nasal passages and upper airways) are compromised. this occurs in intubated patients or in those receiving non humidified high-flow oxygen. • In these situations inspired gases should be humidified routinely.
Fluid and Electrolyte Balance during Injury Insensible fluid losses: Pyrexia • 200ml/day for each 1°C rise in temperature. Sweating • May increase fluid loss by up to 1 litre/hour • Sweat also contains significant amounts of sodium (20-70mmol/l) and potassium (10mmol/l).
Fluid and Electrolyte Balance during Injury The effect of surgery: The stress response • ADH leads to water retention and a reduction in urine volume for 2-3days following major surgery. • Aldosteroneconserves both sodium and water, further contributing to oliguria. • Urinary sodium excretion falls while urinary potassium excretion increases, predisposing to hypokalaemia.
Fluid and Electrolyte Balance during Injury 'Third-space' losses: • if tissue injury is severe, widespread and/or prolonged then the loss of water, electrolytes and colloid particles into the interstitial space can amount to many litresand can significantly decrease circulating blood volume following trauma and surgery.
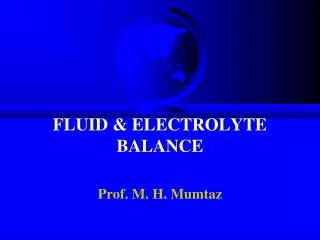
Regulation of Fluid BalanceQ=K[(Pc-Pi)-@(Oc-Oi)] Arteriole Venule Pnet =(37-1)+(0-25)=11 17 Mm Hg 37 mm Hg Oncotic P=25 Interstitial Hydrostatic P=1 Pnet =(17-1)+(0-25)=-9
Fluid and Electrolyte Balance during Injury 'Third-space' losses: • Colloid oncotic pressure throughout the lumen of the capillary is 25mmHg. • The hydrostatic pressure is 1 mmHg in the interstitium. • Hydrostatic pressure on the arteriolar side of the capillary falls from 37 mmHg to 17 mmHg on the venular side. • net outward pressure on the arteriolar side (37 - 1 - 25 = 11) • net inward pressure (25 -17-1= 9) on the venular side.
tending to move fluid out of the capillaries tending to keep fluid within the capillaries Regulation of Fluid Balance Oncotic pressure Hydrostatic pressure Excess fluid filtered is collected through the lymphatic circulation and returned to the Systemic circulation THE STARLING EQUATION
Fluid and Electrolyte Balance during Injury Third-space' losses: • This normal arrangement gets disturbed and oedema is formed ifthe hydrostatic pressure increases on the venularside as in heart failure or the colloid oncotic pressure falls due to liver or kidney disease or the permeability is increased as in sepsis and /or injury.
Fluid and Electrolyte Balance during Injury Loss from the gastrointestinal tract • The magnitude and content of fluid losses depends on the site of loss or lntestinalobstruction. • lngeneral, the higher an obstruction occurs in the intestine, the greater the fluid loss
Fluid and Electrolyte Balance during Injury Loss from the gastrointestinal tract Paralytic ileus. • Propulsion in the small intestine ceases, has numerous causes. • Resolves within 1-2days of the operation.
Fluid and Electrolyte Balance during Injury Loss from the gastrointestinal tract: Intestinal fistula • As with obstruction associated with the greatest fluid and electrolyte losses. As well as volume,
Fluid and Electrolyte Balance during Injury Loss from the gastrointestinal tract: Diarrhoea. • Patients may present with diarrhoeaor develop it during the perioperative period. • Fluid and electrolyte losses may be considerable.
Fluid and Electrolyte Balance during Injury Intravenous fluid administration: When choosing and administering intravenous fluids it is important to consider: • what fluid deficiencies are present. • fluid compartments requiring replacement. • electrolyte disturbances present . • which fluid is most appropriate.
Fluid and Electrolyte Balance during Injury Types of intravenous fluid: • Dextrose • After the IV administration of 1000 ml 5% dextrose solution, about 670ml of water will be added to the intracellular fluid compartment (lFC) and about 330 ml of water to the extra cellular fluid compartment (EFC), of which about 70ml will be intravascular. • Dextrose solutions are therefore of little value as resuscitation fluids to expand intravascular volume
Fluid and Electrolyte Balance during Injury Crystalloids • Sodium chloride 0.9%(NS) and Hartmann' s solution (Ringer) are isotonic solutions • Sodium chloride NS 0.9 contains 9g of sodium chloride dissolved in l000ml of water. • (Ringer's lactate) has a more composition, containing lactate, potassium and calcium addition to sodium and chloride ions.
Fluid and Electrolyte Balance during Injury Crystalloids • Both normal saline and Ringer solution have an osmolality similar to extracellular fluid (about 300m0sm/l) and after venous administration they distribute rapidly to ECF compartment.
Fluid and Electrolyte Balance during Injury • One liter of isotonic saline contains 154 meq of sodium and an equivalent number of chloride ions.