EBB AND TIDE IN HIATUS HERNIA MANAGEMENT
EBB AND TIDE IN HIATUS HERNIA MANAGEMENT. PROFESSOR THARWAT MOHAMED ALY. WHAT IS HIATUS HERNIA ?. PROTROUSION OF A PORTION OF STOMACH INTO THE OESOPHAGEAL HIATUS IT IS A COMMON CONDITION 60 % OF PEOPLE AFTER AGE OF 60 HAVING SOME DEGREE OF HIATUS HERNIA. TYPES OF HIATUS HERNIA.

EBB AND TIDE IN HIATUS HERNIA MANAGEMENT
E N D
Presentation Transcript
EBB AND TIDE IN HIATUS HERNIA MANAGEMENT PROFESSOR THARWAT MOHAMED ALY
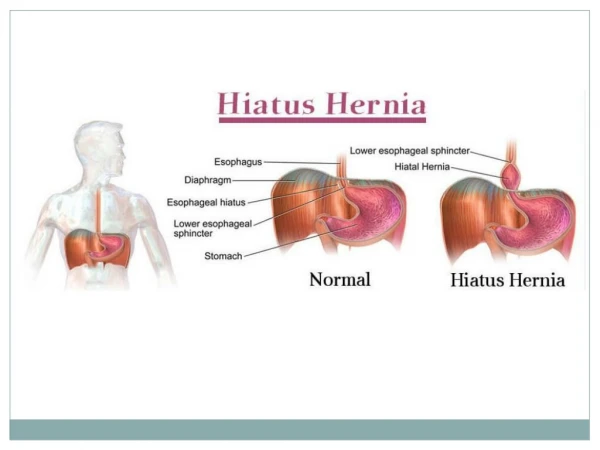
WHAT IS HIATUS HERNIA ? • PROTROUSION OF A PORTION OF STOMACH INTO THE OESOPHAGEAL HIATUS • IT IS A COMMON CONDITION 60% OF PEOPLE AFTER AGE OF 60 HAVING SOME DEGREE OF HIATUS HERNIA
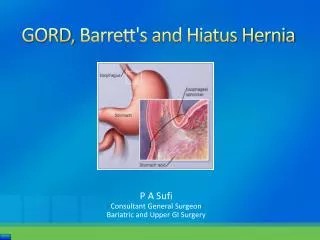
TYPES OF HIATUS HERNIA There are 5 types of hiatal hernia. • Sliding typethe junction between the stomach and esophagus slides up through the esophageal hiatus during moments of increased pressure in the abdomen this type represents 95%of cases • Para-oesophagealwhen a portion of the stomach remains stuck in the chest cavity • Combination of both sliding and para-oesophageal • Sliding of other structure with stomach like omentum spleen or colon • Hiatus Hernia after Bariatric surgery
Type 1 Type 2
CAUSES OF HIATUS HERNIA • Obesity • Smoking • Alcohol • Increased intra abdominal pressure • Repeated Pregnancy • Straining • Coughing…etc. • Frequent Bending during lifting heavy weights • Hereditary weakness of sphincter
CLINICAL PICTURE • Silent • Symptoms of GERD as: • Heart pain, chest pain, belching and bloating • coughing or hiccough, feeling of food stuck to lower part of esophagus • Dysphagia • Emergency in Paraoesophageal type as: • Acute epigastric or chest pain, difficulty in swallowing • Stomach pain due to strangulation of ParaoesophagealHernia
Diagnosis • Clinical presentation • Plain x ray chest
ENDSCOPY HAS THE MOST IMPORTANT ROLE FOR DIAGNOSIS WHY? • To diagnose presence of hernia? • To diagnose presence of GERD in some cases? • To diagnose Barrett’s? • In some cases as treatment? • Non of the above? • All of the above?
IF ENDSCOPY IS NORMAL WHAT TO DO TO DIAGNOSE PRESENCE OF GERD? • TAKE MULTIPLE BIOPSIES IN THE AREA 2CM ABOVE Z LNE ? • DO OTHER INVESTIGATIONS LIKE pH METRY OR MOTILITY STUDY?
IMPORTANCE OF BIOPSIES IN NORMAL ENDSCOPY • IT CAN DIAGNOSE PRESENCE OF OESOPHAGITIS • BY PRESENCE OF HISTOLOGICAL CHANGES OF • MUCOSA IN MORE THAN 70% OF PATIENTS WITH • HIGH SPECIFICITYMORE THAN 80%
Motility and pH study Indications: • Patients with gas bloat syndrome? • Motility disorders ? • Patients with regurgitation and choking? 4- Negative endoscopy with typical symptoms? 5-Atypical presentation ? 6-All of above?
Medical Treatment • 1- CHANGE LIFE STYLE A-Losing weight, if overweight B-Decreasing the size portions of meals C-Avoiding certain acidic foods D-Limiting fried and fatty foods, foods containing caffeine -Eating meals at least three to four hours before lying down, and avoiding bedtime snacks F--Keeping your chest six inches higher than the rest of your body when lying on your back. Raising the level of your head helps gravity keep your stomach’s contents in the stomach. G--Quitting smoking H--Not wearing a tight belt or tight clothing that can increase the pressure on the abdomen • 2- MEDICAL TREATMENT MANLY BBI AND OTHER DRUGS
INDICATIONS OF SURGERY • Sliding hernia with GERD … especially in patients with • Side effects of medical treatment • Non compliance with medical treatment • Socioeconomic factors • Non acid reflux with Sliding hernia • Sliding hernia with atypical symptoms with consent of 30% failure 4-Type 111 Hiatus hernia 5-Incarcerated para-oesophageal hiatus hernia
IS ANTIREFLUX SURGERY STILL PERFORMED FREQUENTLY AS IN THE PAST? • Yes? • No?
Number greatly decreased IN US BY 30% due to • PROPER PATIENT SELECTION? • BETTER UNDERSTANDING OF THE GERD PROBLEM? • BETTER DIAGNOSIS? • IMPROVEMENT IN ENDSCOPIC MANAGEMENT? • MEDICAL TRATMENT WITH BBI?
Crural repair • Always posterior? • Posterior and anterior? • Mesh repair? 4-All of the above are valid options?
DIVISION OF SHORT GASTRIC • YES? • NO?
TYPE OF REPAIR • Nissen’s fundoplication ? • Toupet repair ?
ANSWER Always Floppy Nissen except: • Not in patients with hypomotility • Not in patients with gass bloat syndrome C-not in-patients with vomiting
USE OF BOUGIE • Always? • Sometimes? • Never?
ANSWER • Advised to pass BOUGE 40 before or after repair
Hiatus hernia with suspected Barrett’s Oesophaguswhat to do ? • Do biopsy first? • Treat Barriett’s first? • Do anti reflux surgery?
Role of surgery in presence of Barrett’s • No Dysplasia or no barrett” • Low grade Dysplasia • High grade Dysplasia
Large hiatus hernia Hiatel Defect by endscopy or at surgery • 1-3 cm defect? • 2-4 cm defect? • 3-5 cm defect?
How to repair huge hiatus hernia • Mesh repair? • No mesh?
Mesh repair • Type of mesh used • Fixation of mesh
DYSPHAGIA • Endoscopic Dilation • Redo surgery
GAS BLOAT SYNDROME • Send to medical doctor, minimum improvement expected • Role of surgery
RECURRENCE OF SYMPTOMS NOT RESPONDING TO TREAT • Redo Surgery? • What to do?
Hiatus hernia with bile reflux How to diagnose 1-Endoscopy ? 2-pH Metry ? 3-Technetium study?
Role of endoscopy in management of hiatus hernia • No role? • Some cases? • Great role?
Role of endoscopy 1-endoscopic trans oral fundoplication using staplers guided by ultrasonography to staple stomach fundus to oesophagus above z line MUSE 2-endoscopic full thickness plication 3-use of radiofrequency Stretta 4-antireflux mucosectomy
Hiatus hernia with bile reflux what to do? • Medical treatment? • Surgery ?
TYPE OF SURGERY IN BILE REFLUX • Nissen fundoplication? • Diversion?