Reflux and hiatus hernias
Reflux and hiatus hernias. Mr Will Hawkins FRCS DipMedEd Consultant Surgeon St Richard’s Hospital & Chichester Nuffield Hospital. introduction. Biography Understanding the jargon What is reflux? Investigating symptoms Non-surgical treatment options Surgery for reflux and hiatus hernias

Reflux and hiatus hernias
E N D
Presentation Transcript
Reflux and hiatus hernias Mr Will Hawkins FRCS DipMedEd Consultant Surgeon St Richard’s Hospital & Chichester Nuffield Hospital
introduction • Biography • Understanding the jargon • What is reflux? • Investigating symptoms • Non-surgical treatment options • Surgery for reflux and hiatus hernias • Conclusions
Biography • Grew up in Cardiff • Trained at the University of Birmingham • Basic and Higher Surgical Training in the West Midlands • Fellowships in Taunton and Sydney specialising in Upper GI and Bariatric surgery • Appointed as consultant at St Richard’s Hospital 2013 • Formerly Sub-Dean Brighton and Sussex Medical School • Surgical Clinical Tutor Western Sussex Hospitals • Training Programme Director for General Surgery in Kent, Surrey & Sussex
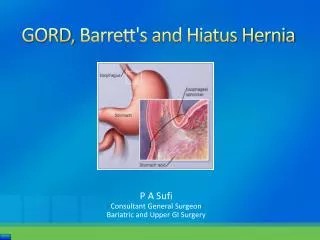
Gastro-Oesophageal Reflux Disease • GORD or ‘reflux’ • Movement of stomach contents into the oesophagus/gullet • Food • Gastric acid • Bile
Non-Erosive Reflux Disease • NERD • GORD without evidence of damage to the gullet at endoscopy • This accounts for a vast majority of patients with GORD
oesophagitis • Inflammation of the gullet • Approximately two thirds of patients have no evidence of this at endoscopy • Approximately two thirds of patients with oesophagitis have no symptoms of reflux
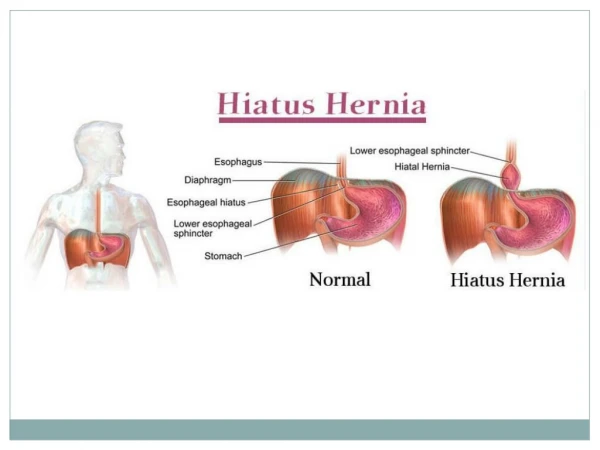
HERNIA • Protrusion of an organ or fatty tissue through a gap in a muscle • The gap may be acquired (e.g. umbilical, incisional or a direct inguinal hernia) or an abnormally large natural defect (e.g. hiatus or indirect inguinal hernia)
(Oesophageal) hiatus • A naturally existing gap in the diaphragm (the muscle separating the chest and abdomen that moves during breathing) that the gullet travels through to reach the stomach
Proton pump inhibitors • Medications that suppress the production of acid in the stomach • Examples: • Omeprazole (Losec) • Lansoprazole (Zoton/Fastab) • Esomeprazole (Nexium) • Pantoprazole (Pantoloc) • Rabeprazole (Pariet) • These should be taken about 30 minutes before eating because eating leads to acid production • Usually on waking • If symptoms worse at night take before the evening meal • Can be taken twice a day
H2 antagonists • Similar drugs that work in a different way • Cimetidine – first drug that really offered a treatment for stomach ulceration • Ranitidine (Zantac) the only one widely available now • Generally less effective but an option for those who can’t tolerate PPIs or for whom PPIs are ineffective
GORD • Reflux is a normal phenomenon but usually cleared rapidly by the gullet after swallowing • Becomes a problem when symptomatic, especially when severe/distressing • Heartburn • Abdominal pain • Regurgitation (volume reflux) • Associated problems • Oesophagitis / Barrett’s Oesophagus / Oesophageal cancer • Cough / Laryngitis / Asthma / Fibrotic (scarring) lung disease • Dental erosion • Approximately 15% of the UK population experience some reflux symptoms on a weekly basis
Causes of gord • Weak lower oesophageal sphincter • Group of muscles at bottom of gullet that usually only relax during swallowing • Hiatus hernia • Widening of the oesophageal hiatus allowing the stomach to slip into the chest • Other disruption of anatomy (angle of His) • Slow stomach emptying
Things that influence gord • Age • Pregnancy • Lifestyle • Smoking, alcohol intake, diet • Obesity • Diabetes • Other medical conditions or their treatment • Heart, gastrointestinal or psychiatric illness • Family history of GORD
Things that mimic reflux • Achalasia • Very high pressure lower oesophageal sphincter that leads to a disordered swallowing movement • Hypersensitive oesophagus • NERD with no demonstrable acid reflux • Oesophageal cancer • Obstruction in the stomach or further along the gut • Other causes of chest pain (e.g. angina, lung disease or musculoskeletal pain)
belching • Not a symptom of reflux but can be a consequence of it • The air is almost always swallowed (unless drinking excessive fizzy drinks) • Dry swallowing is a learned reflex often to alleviate the symptoms of reflux (as this clears the gullet of the refluxed material) • This can be difficult behaviour to reverse • Bloating is likely to be due to the same mechanism but can also be a symptom of Irritable Bowel Syndrome (IBS) that often co-exists
investigations • Most patients do not require investigation initially • Trial of PPI • If fails or symptoms recur after the initial course warrants investigation • Upper GI Endoscopy usual initial investigation • Other investigations warranted if contemplating surgery, if symptoms are severe or there is a large hiatus hernia • Oesophageal manometry and pH studies • CT or barium swallow
endoscopy • NICE recommendations • Urgent endoscopy: • Significant Upper GI bleed • Swallowing difficulties (food getting stuck in lower gullet +/- regurgitation) • Reflux and weight loss if over 55 years old • Routine endoscopy: • Reflux unresponsive to PPIs • Reflux with associated anaemia or vomiting
Endoscopy (OGD) • Simple, quick investigation • Allows visualisation of the oesophagus, stomach & duodenum, usually several photos taken • Biopsies taken if anything found or to look for H pylori • Usually well tolerated • All patients have throat spray • Entonox (gas & air) and sedation (midazolam) options if not tolerated • Rarely general anaesthetic is required
Oesophageal manometry • Performed in those with suspected achalasia or those considering antireflux surgery (to ensure no contra-indication) • Involves a catheter inserted through the nose into the gullet • The patient swallows 10 sips of water • The catheter measures gullet pressures during swallowing
Oesophageal pH studies • The nasal catheter is replaced with a finer catheter with a pH probe at its tip • The tip is positioned in the lower oesophagus and left for 24 hours • The patient is asked to have a ‘bad day’ • Off medication for 2 weeks beforehand • Do things that usually cause symptoms • Symptoms are recorded and compared to the amount of acid (the pH level) recorded by the probe • A good correlation is required to contemplate surgery
Other oesophageal studies • BRAVO • A capsule placed endoscopically that can monitor pH levels without requiring a nasal catheter • It eventually falls off the gullet wall and passed in the stool • Oesophageal impedance • Similar to pH studies but monitors fluid in the gullet • Used to diagnosis non-acid reflux • Occasionally offered if patients cannot tolerate coming off their medication for pH studies
Hiatus hernia • Type I (sliding) most common and often related to reflux • Other types, especially Type IV, associated with other symptoms • Vomiting • Anaemia • Pain on eating • Prolonged fullness after eating • Can present as an emergency with severe pain due to excessive twisting
Initial treatment • Over the counter remedies • Gaviscon, Rennie, etc • Lifestyle modification, avoiding causative factors
Medical therapies • Some available over the counter but usually best monitored by the GP • PPIs • H2 antagonists • Prokinetics – medications that encourage stomach emptying • May be recommended after an endoscopy, usually if bile is seen refluxing into the stomach and may be causing symptoms by also refluxing into the gullet • Only for short term use due to side effects if used long term • Domperidone – heart rhythm abnormalities • Metoclopramide – movement disorders or mental health disturbances
Are ppis safe? • PPIs are very commonly prescribed but are often a source of headlines in the press • All medications have the potential to cause side effects or harm • Overall PPIs are safe medications • Not everyone can tolerate PPIs and some experience GI disturbance (such as diarrhoea). If one type is not tolerated, others often are. • Long term acid suppression will have an effect on the absorption of some nutrients, most notably calcium. There is a recognised link to PPI use and osteoporosis. • PPIs use is associated with a slight increase in stomach cancer but a more profound decrease in the more common oesophageal cancer • The most powerful research studies have shown no link with PPIs and cardiac disease
Surgery & other interventions • Laparoscopic (keyhole) fundoplication +/- hiatus hernia repair • Open surgery • Novel interventions • LINX – magnetic ring placed around the lower part of the gullet • Stretta – endoscopic heating (radio-frequency ablation) of the lower oesophagus to strengthen the lower oesophageal sphincter mechanism
Anti-reflux surgery • The only intervention that can truly offer a CURE for GORD • Prior to surgery • Need to objectively demonstrate that symptoms are due to reflux • Endoscopy • pH studies (& manometry to ensure no contraindication due to a motility problem)
The operation • Admitted on day of surgery • General anaesthetic • 5 x 5mm incisions (one may be 10mm if reinforcement material used) • Procedure • Assess anatomy • Dissect fully around the bottom of the gullet/repair any hiatus hernia • Wrap part of the stomach (the fundus) around the bottom of the gullet • Usually home the following morning • Post-operative diet – 2 weeks each of fluids / pureed / mash
variations • Usually surgeon preference (based on their training/experience) or patient preference • All offer benefit in clinical trials • Provides options if one fails to control reflux or proves to be too ‘tight’ • However, redo surgery usually more challenging and higher risk
Reinforcement of large hiatal defects • Tissue around hiatus hernias can be weak (especially of large hernias) • Repair with sutures can leave a high risk of recurrence • Early recurrence of a hiatus hernias tends to be associated with more severe symptoms • Risk of plastic (usually Nylon) meshes • Bioabsorbable meshes are now available • Promising early results but there is no long term data yet • They do appear to reduce short-term recurrence rates without any major complications
Bio-A tissue reinforcement • Material consisting of a web of absorbable synthetic polymers • Used in the repair of recurrent or large hiatus hernias • Mechanical barrier in the initial healing phase • Stimulates the production of stronger scar tissue • Can also be used when the hiatus cannot be fully closed but will usually require further surgery to further repair the hiatus in the future
Risk vs benefit • Advantages • Offers potential of long term cure of reflux symptoms • Can usually return to normal activities (eating, sleeping, etc without medication) • Disadvantages • Major operation (albeit now as a low pain, keyhole procedure) • Reduced dietary intake for several weeks often with associated weight loss • Potential to develop ‘gas bloat’ – related to difficulty belching (+/- vomiting) • Rarely major complications from surgery • Potential of recurrent symptoms, although at 10 years > 90% of patients remain satisfied with their outcome
Who can have surgery? • Patients suitable for surgery • Patients with severe symptoms – especially volume reflux • Patients with complicated disease – e.g. associated lung disease or Barrett’s oesophagus • Patients intolerant to medication for reflux or for whom medication is ineffective • Patients with good control who would prefer not to have long term medication • Could be argued that ALL patients with symptomatic reflux should at least be considered for surgical correction if medically fit for surgery • It is very much a question of PATIENT CHOICE
Type iv hiatus hernia • Type IV or para-oeosphageal hiatus hernias are often associated with more severe symptoms • Risk of volvulus (twisting of the stomach which can affect the blood supply) • Surgical repair is recommended to all patients with such hernias that are symptomatic • However, these are often frail, elderly patients for whom a watchful approach may be more appropriate
conclusion • Reflux and hiatus hernias are common problems • Symptoms can often be controlled with lifestyle modifications • Safe and effective medication is available but may require long term treatment • Surgery is an option is medication fails or for those who would prefer not to take medication • Surgery offers the potential for long term cure and is generally safe surgery • Novel quasi-surgical options are available but remain largely experiemental