Download
1 / 40
440 likes | 671 Vues
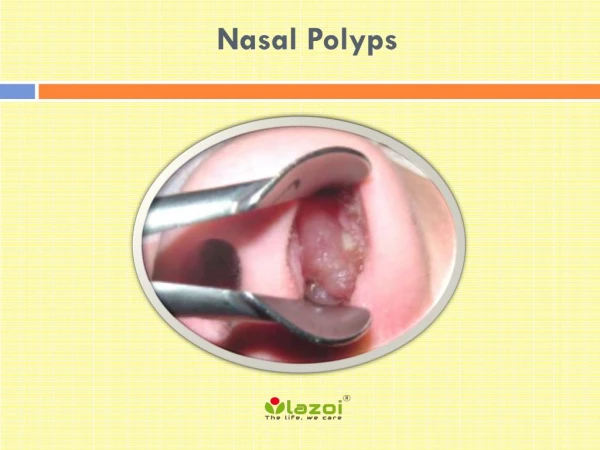
Nasal Polyps - Pathogenesis and Treatment Implications. Bastaninejad , Shahin , MD, Assistant Professor of ORL-HNS, TUMS, Amir’Alam Hospital. Importance. NPs have been shown to have a significant detrimental effect on the quality of life , which is similar in severity to COPD.

E N D
Nasal Polyps - Pathogenesis and Treatment Implications Bastaninejad, Shahin, MD, Assistant Professor of ORL-HNS, TUMS, Amir’AlamHospital
Importance NPs have been shown to have a significant detrimental effect on the quality of life, which is similar in severity to COPD
Introduction • Nasal polyps appear as grape-like structures in the upper nasal cavity, originating from within the ostiomeatal complex • They consist of: loose connective tissue, oedema, inflammatory cells and some glands and capillaries, and are covered with varying types of epithelium, mostly respiratory pseudostratified columnar epithelium…
Eosinophilsare the most common inflammatory cells in nasal polyps (80%), but Neutrophils, mast cells, plasma cells, lymphocytes and monocytes are also present, as well as fibroblasts • IL-5 is the predominant cytokine in nasal polyposis, reflecting activation and prolonged survival of eosinophils
In the general population, the prevalence of nasal polyps is 4% (2.2/1 MF Ratio) • The average age of onset is approximately 42 years • In patients with asthma, a prevalence of 7 to 15% has been noted whereas, in NSAID sensitivity, nasal polyps are found in 36 to 96% of patients
Factors associated with NP • Allergy Only Kern state inhalant allergy as a risk factor for NP, but food allergy is significantly higher in NP patients (80%) • Asthma NPs are present in 13% in non-atopic asthma (skin prick test and total and specific IgE negative) and 5% in atopic asthma • Aspirin sensitivity In patients with aspirin sensitivity 36-96% have nasal polyps
Factors associated with NP • Genetics NP are frequently found to run in families… HLA-A74 , HLA-DR7 • Environmental factors The role of environmental factors in the development of NP is Unclear
Hypotheses regarding the underlying mechanisms • Chronic infection (Fungal/Bacterial) • Aspirin intolerance (Samter) • Aerodynamics alteration with trapping of polutions • Epithelial cell defects / Epithelial disruptions • Gene deletions (CFTR genes in CF) • Inhalant or food allergens (discussed in previous page)
Chronic Rhinosinusitis Nasal Polyps The spectrum of sinus disease Nasal Polyps Chronic rhinosinusitiswith and without nasal polyps 20-33% of CRS Rhinosinusitis PMNEOS TH1TH17TH2 (INF-gama, IL-8) (IL-4, IL-5)
Histopathology • Frequent epithelial damage, a thickened basement membrane, and Edematous to sometimes fibrotic stromal tissue, with a reduced number of vessels and glands but virtually no neural structure • Among the inflammatory cells, Eosinophils are a prominent and characteristic feature in about 80% of polyps
H&E staining . Immunoperoxidase staining
Pathomechanism • Eosinophilic inflammation • IL-5 was found to be significantly increased in nasal polyps • Cytokine IL-5 Eos ECP (E. cationic protein) progression in pathology
Pathomechanism • Extracellular matrix regulation • Eos TGF-β1&2 Fibroblast activity progression in pathology (increase in extra cellular matrix formation)
Pathomechanism • Role of Staphylococcus aureus enterotoxins (SAE) • Multiclonal IgE antibody formation to SAE can be seen in nasal polyp tissue, but rarely in CRS • It is positive in about 30-50% of the patients with NP and in about 60-80% of nasal polyp subjects with asthma
Epithelial damage (barrier dysfunction) Hyper IgE Cytokines Polyclonal IgE chronic microbial trigger Albumin Superantigens Eosinophils ( apoptosis) IL-5 Chemokines Eotaxin ECP T B Nasal polyposis: aetiology and pathogenesis S. Aureus enterotoxins: disease modifiers
Demo for Pathogenesis polyps B cell Mast cell eosinophil Y Y Y Y Arachydonic acid cytokines Y Y Y Cycloxygenase 5 lipoxygenase Leukotrienes Prostaglandin Histamine Interleukin Thanks from Dr. R. Cathcart for this demo
Differentials • Encephalocoeles • Gliomas • Dermoid tumours • Haemangiomas • Papillomas / transitional cell papillomas • Nasopharyngeal angiofibromas • Rhabdomyosarcomas • Lymphomas • Neuroblastomas • Sarcomas • Chordomas • Nasopharyngeal carcinomas
Medical Treatments • Corticosteroids • reduce airway eosinophil infiltration by preventing their increased viability and activation • Directily • Or via reducing the secretion of chemotactic cytokines by nasal mucosa and polyp epithelial cells • Topical Cort.: effect on poly size and also on symptoms associated with NP such as nasal blockage, secretion and sneezing but the effect on the sense of smell is not high
Postoperative treatment with topical corticoidsteriods • Postoperative effect on recurrence rate of NP after polypectomy with intranasal steroids is well documented and the evidence level is Ib • But in patients who undergone FESS operation did not showa positive effect of local corticostoroids over placebo (3mo-1yr-2yr)
Systemic steroids : • Is effective in polyp reduction and nasal symptoms associated with NP, even on sense of smell • Oral corticosteroids for 10 days (20-40mg) there are reports with 21 days and also higher doses (up to 50mg) of prednisolone • The benefit of oral steroids, however, remains less definitive with little randomized data available and the risk of systemic effect from oral steroids use in severe cases
Antibiotics: • There is also increasing evidence in vitro of the anti-inflammatory effects of macrolides • The exact mechanism of action is not known, but it probably involves down regulation of the local host immune response as well as a downgrading of the virulence of the colonizing bacteria
Regimens (12wk also you can try 6wk): • Erythromycin Ethylsuccinate: 400 q6h up to 2wk, then 400 q12h up to 10wk • Clarithromycin: 500 q12h up to 2wk, then 500 daily up to 10wk • AZM 2011 lack of efficacy in treatment of CRS with or without NP
Antihistamines: • Cetirizine in a dose of 20 mg/day for three months, significantly reduced sneezing, rhinorrhoea and obstruction compared to placebo but with no effect on polyp size • So it is recommended in allergic patients with NP
Antileukotrienes: • There are a few case controlled trials indicate that antileukotriene treatment may have beneficial effect on nasal symptoms in patients with chronic/persistent rhinosinusitis and nasal polyposis
Capsaicin: • It is a neurotoxin that depletes substance P with some other neurokinins and neuropeptides, leading to long-lasting damage to unmyelinated axons • Tested in Eosinophilic non allergic non asthmatic NP • capsaicin significantly increased NSAV (nose-sinuses air volume) and very significantly improved subjective and endoscopy scores, but did not significantly alter ECP
Method of Capsaicin delivery: • for 3 consecutive days patients received: 0.5 ml 30 mmol/L capsaicin solution sprayed into each nostril, and 100 mmol/L of capsaicin solution on days 4 and 5, respectively
Furosemide: • It exhibited an anti-inflammatory effect • Also it acts on Na/Cl transporter and reduce tissue edema, too • Passali (2003) - RCT-n=177, post polypectomy furosemide vs. placebo vs. mometasone. Results after 5yr F/U: 17% recurrence with furosemide 30% recurrence with placebo 24% recurrence with mometasone
Method of furosemide delivery: • Furosemide diluted in physiological solution (2 ml of furosemide in 2 ml of saline) administered as nasal puffs (2 puffs per nostril a day, each puff corresponding to 50 micg) for 30 days. • Frist 2yrs: every other mounth (12/24mo) • Next 2yrs: 1mo on, 2mo off (8/24mo) • In 5thyr: 2mo in a year (2/12mo)
Strength of evidence for treatment of CRS vs. NP InterventionChronic rhinosinusitisNasal polyps Corticosteroids Topical A A Systemic / C Antibiotics Oral short term < 2w C D Oral long term (12w) C C Antimycotics Topical / Systemic D D Antihistamines D B Anti-leukotrienes / C Nasal saline douche C D Decongestants D D Allergen avoidance D D
Guideline in our country • INCS for undisclosed time ? • Macrolide administration for 6 to 12wks • Oral corticosteroids for 10-20 days (20-40mg) • Montelukast (10mg/day) • In allergic patients: Cetrizine 20mg/day for 3mo
2 3 1 5 Scheme for experimental polyp treatment polyps B cell Mast cell eosinophil Y Y Y Y Arachydonic acid cytokines Y Y Y Cycloxygenase 5 lipoxygenase Leukotrienes Prostaglandin Histamine Interleukin 4
Anti IgE Anti IL-5 Future therapies in nasal polyposis Anti-CCR3? Anti-IgE? Eotaxin IgE Tacrolimus? Anti-IL-5? IL-5 Corticosteroids? Anti-LTs? ECP Antibiotics?Anti-fungal?
Surgical Treatments • Surgical treatments, including Polypectomy alone or in combination with FESS, rarely result in long term control of polyposis and are typically combined with medical treatment • When hyposmia is the primary symptom, no additional benefit seems to be gained from surgical treatment. If nasal obstruction is the main problem after steroid txy, surgical treatment is indicated
When to proceed with surgical therapy? • when medical therapy fails to control symptoms • when the patient is not suitable for oral steroids • when total nasal obstruction occurs • when there is persistent infection or complications
Simple polypectomy vs. FESS!? Dalziel (2003) - meta-analysis : Symptom improvement Recurrence FESS 78-88% 28% Simple 43-84% 35% 7% difference!!
When is it logical to perform FESS instead of a simple polypectomy operation? • Severe and extensive disease • Underlying diseases (Asthma, Samter, Allergic fungal, CF,…) • Revision cases when pathology is not localized
Thank You! Bastaninejad MD