Download
1 / 38
390 likes | 463 Vues
Explore the spectrum of pituitary diseases, from adenomas to tumour types, along with genetic advances and familial predispositions. Learn about hormonal effects, diagnostic imaging, and current therapeutic approaches in pituitary tumour therapy.

E N D
Pituitary disease Prof Julian Davis Endocrinology Group, School of Biomedicine, University of Manchester Department of Endocrinology, Manchester Royal Infirmary
Hypothalamic-pituitary hormone axes Hypothal Pituitary hormone - cell Target hormone CRH ACTH - corticotroph cortisol TRH TSH - thyrotroph thyroxine GnRH LH - gonadotroph T, E2 GnRH FSH - gonadotroph inhibin GHRH GH - somatotroph IGF-1 DA Prolactin - lactotroph
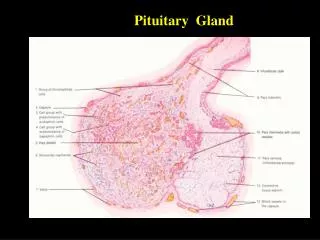
Normal pituitary gland: cell types intermingled ACTH – corticotrophs TSH - thyrotrophs LH, FSH - gonadotrophs GH - somatotrophs Prolactin - lactotrophs Normal pituitary - mixed cell types
Pituitary adenomas Benign, slow-growing Differentiated Local expansion Incidental small tumours common Mass effects - headache, visual loss Hormonal effects - hormone overproduction
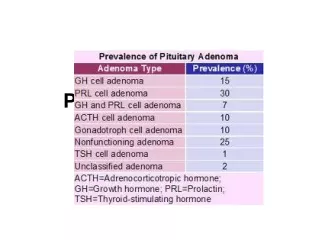
Pituitary tumour types Differentiated tumours containing single pituitary cell types Lactotroph: PRL prolactinoma Somatotroph: GH acromegaly Corticotroph: ACTH Cushing’s disease Gonadotroph: LH, FSH = non-functioning Thyrotroph: TSH
Investigation: pituitary imaging CT scan: axial coronal Lateral skull X-ray
Functioning clonal tumours give endocrine syndromes: PRL excess (prolactinoma) – lactation, amenorrhoea Amenorrhoea Hypogonadism Infertility Galactorrhoea
GH excess: gigantism and acromegaly GH excess Soft tissue and bone growth Tall stature Enlarged face, hands, feet… Metabolic effects: BP, diabetes…
Non-functioning adenomas LH/FSH gonadotroph adenomas: LH or FSH excess rare… usually just α- or ß-subunits, no endocrine effect, hence ‘non-functioning’ → mass effect & hypopituitarism TSH thyrotroph adenomas: TSHoma = very rare cause of thyrotoxicosis
Craniopharyngioma • Rare benign tumours • Remnants of Rathke’s pouch • Solid tissue, cysts, • calcified nodules • Within or above the pituitary
Pituitary tumour pathogenesis • Little definite conclusive evidence • Hormonal environment can predispose to tumours: • oestrogens can induce prolactinoma in rats • D2R knockouts get prolactinoma • NGF overexpression causes prolactinoma • reversible ‘trophic changes’ in pituitary populations may lead to overgrowth of clonal populations? • Intrinsic genetic alterations lead to clonal expansion • gsp mutation can ‘explain’ 40% of Ghomas • no other characteristic mutations identified
Genetic advances – familial pituitary adenomas • MEN-1 • Menin gene 11q13 • Carney Complex • PRKAR1A, 17q22-24; 2nd locus… • McCune-Albright • Gsp oncogene • Familial predisposition syndrome • AIP
Familial adenoma predisposition:discovery of AIP Two extended families, northern Finland Two clusters linked as 1 family by genealogy (generation I from 1700s): 3 cases of acromegaly/gigantism Low penetrance familial adenoma predisposition to PRLoma and GHoma Whole-genome SNP genotyping done on 16 individuals Linkage to 11q13, but no MEN1 mutations AIP gene identified, mutations in cases Vierimaa et al, Science 2006
AIP: Aryl hydrocarbon Interacting Protein • AIP 330 amino-acids • FKBP-homology domain • 3 tetratricopeptide repeats (TPRs) • AIP complexes with aryl hydrocarbon receptor (AHR) and Hsp90 • (AHR = ligand-activated TF) • AIP also binds and impairs function of phosphosdiesterase PDE4A5 and PPAR • Mutations render AIP inactive; • many AIP-assoc adenomas null for AIP protein A. Normal pit; B. AIP-proficient adenoma C-D: acromegaly, AIP Q14X mutation, -ve ICC Georgitsi et al, PNAS 2007
Natural history • Autopsy and scanning data • Autopsy(meta-analysis by Molitch, 1997) • Variable rates: 1-27%, average 11% • males=females • 3 / 1403 are macroadenomas • 46% stained for prolactin • Scanning: • CT: >3mm adenomas in 4-20% (Molitch, 97) • MR: 10 / 100 if 2 reviewers agreed, 25-48 / 100 if one only (Hall, 94)
Natural history • Long-term follow-up • 156 patients followed over 8y (Molitch, 1999) • tumour expansion in 6% • PRL levels stable or fell in 75% • i.e. prolactinomas may be very indolent, may remit, may not need treatment • Worth a trial of withdrawal of drug treatment
Pituitary tumour therapy Surgery Radiotherapy Drug therapy DAs Somatostatin analogues GH antagonists
Transsphenoidal pituitary surgery • Potential for long-term cure and avoidance of DA side-effects • Outcomes poor for PRLomas even in specialist hands - 50-75% long-term endocrine remission for microadenomas
Endoscopic transphenoidal surgery – Manchester experience 2005-2007 125 consecutive patients endoscopic approach single surgeon Comparison of two consecutive 15 month periods 05-0606-07total NF adenomas 22 45 67 Acromegaly 15 7 22 Cushing’s 4 6 10 PRLoma 6 3 9 Cranio 2 2 4 Apoplexy 1 5 6 Macroadenoma 40 66 106 Surgical duration 120 91 101 Hospital stay 7 (3-36) 4 (3-15) 5 Leach et al, Neurosurgery, 2010
Endoscopic surgery - outcomes 61 (49%) had VF deficits … improved in 54 unchanged/worse in 7 Endocrine remission Acro 12/15 6/7 18/22 (82%) Cush. 2/4 5/6 7/10 Hypopit 17% 25% 22% New DI 4% 6% 5% Complications 9% (CSF leak/meningitis, sphenoid sinusitis…) Reoperations 15% (CSF leak, residual tumour) Leach et al, Neurosurgery, 2010
Radiotherapy Prevents tumour regrowth Slow effect Gradual hypopituitarism, Over 10-15 years
Role of radiotherapy • Often used post-op after ‘non-curative’ surgery • Progression-free 15y survival: • 93% after RT • 33% for non-RT
Dopamine agonists • Bromocriptine • introduced 1971 • reduces prolactin in 85-90% • restores gonadal function in 80-90% (women) • significant tumour shrinkage in 80% • mostly in first 3 months, but effect continues • useful shrinkage in 24-48h • Cabergoline, Quinagolide • introduced 1990s • similar PRL response rate • similar adenoma shrinkage rate
Bromocriptine: PRL suppression 55y female PRL 656,000mU/L (NR 100-500) BCR treatment only
Cessation of dopamine agonists: prospective study - Colao et al, (2003) NEJM, 349:2023 • 200 patients 25 non-tumoral • 105 microprolactinoma • 70 macroprolactinoma • -stable on cabergoline, PRL suppressed to normal (25µg/L; 550mU/L) • -small tumour residue, or no residue • Cabergoline withdrawn after 2-5y: recurrence rates… • Non-tumoral hyperprolactinaemia 24% • Microprolactinoma 30% • Macroprolactinoma 36% • possibility of permanent remission, even for macroadenomas • chances better if scan showed no tumour residue • caution for longer term follow-up, but worth trial withdrawal • follow-up study (Clin Endo 2007): PRL and tumour size criteria
Is acromegaly different? SSTRs: receptor targets for medical therapy of GH tumours 5 SSTRs cloned 1990s – wide tissue distribution SSTR-2 and SSTR-5 most highly expressed in pituitary
Somatotroph tumours: modest shrinkage with long-term somatostatin agonists Acromegaly: MRI assessment of primary octreotide therapy 25 patients: 76% showed >25% of tumour shrinkage, after 6 months of treatment. Tumour shrinkage: Mild in 40% - IGF1 normalised in 5/10 Moderate in 24% - IGF1 normalised in 4/6 Remarkable in 12% - IGF1 normalised in 3/3 Figure shows a patient who achieved 75% of tumour shrinkage, but no IGF-I/GH normalization. Jallad, Bronstein et al, Clin Endo 2005
Pituitary tumour shrinkage – response varies Prolactinomas - dramatic shrinkage in 80%+ with dopamine agonists - change in size with oestrogen (more marked in rodent models) Somatotrophinomas - mild-moderate slow shrinkage in ~50% with somatostatin analogues Gonadotroph adenomas – little evidence: eg 7/13 showed 10% shrinkage with long-term dopamine agonist (Lohman, Pituitary, 2001) Review - 5/100 shrinkage with octreotide in 11 studies - 55/199 shrinkage with DAs in 24 studies (Colao, Endo Rel Cancer, 2008) Corticotroph adenomas – no evidence Mechanism – the plastic pituitary, or the plastic lactotroph? Apoptosis in PRLomas? – increased reticulin staining in surgical specimens after DAs Alteration in lactotoph cell size vs cell number?
Clinical databases for measuring and understanding outcomes • UK National Acromegaly Register • Established 1997 • 22 centres • 1920 patients • Outcomes analysis: • Radiotherapy study, 1840 patients • Jenkins et al, JCEM 2006 • Transsphenoidal surgery outcomes, 785 patients • Bates et al, Clin Endo 2007
Acromegaly surgical outcomes ‘safe’ GH 1319 patients underwent TS surgery; 1185 as primary treatment; Interpretable GH data in 785 Interpretable IGF-1 data in 430 Variation in success rates: 20-68% among centres with >10 cases; Overall ‘safe GH’ rate 39% normal IGF-1 Bates et al, Clin Endo, 2007
Surgery for acromegaly: trend for improving results: pre-1985 to 2004 Messages: Increased scrutiny of outcomes by colleagues and patients Improving practice, fewer more specialised pituitary surgeons Stated desirable case-loads (>20 functioning tumours/year)
Summary • Pituitary tumours: benign, indolent, locally destructive. • Cell type of origin determines clinical picture (prolactinoma, acromegaly, Cushing’s, non-functioning etc) • Pituitary adenoma pathogenesis becoming better understood, but still few candidate genes for sporadic adenomas • Natural history of disease more variable than thought – remission occurs • Therapy and outcomes undergoing more scrutiny – role of disease databases