Fecal Incontinence
Fecal Incontinence. Seema Izfar. 2/29/12. Fecal Incontinence. affects estimated between 2-20% people, 50% nursing home residents at risk: parous females, cognitively impaired, elderly defined as “recurrent uncontrolled passage of fecal matter for at least one month”

Fecal Incontinence
E N D
Presentation Transcript
Fecal Incontinence • Seema Izfar 2/29/12
Fecal Incontinence • affects estimated between 2-20% people, 50% nursing home residents • at risk: parous females, cognitively impaired, elderly • defined as “recurrent uncontrolled passage of fecal matter for at least one month” • “partial incontinence” - inability to control flatus or fecal soiling
Etiology • continence: anal sphincters, pelvic floor, stool volume/consistency, rectal compliance, neurological function • pseudo-incontinence: hemorrhoidal prolapse, incomplete evacuation, poor hygiene, STDs, neoplasms, IBD • fecal urgency vs. incontinence • overflow incontinence
Obstetrical Trauma • anal sphincter injury • occult obstetrical injury in 25- 35% of vaginal deliveries (!!!!!!!!!!) • risk factors: forceps, episiotomy, primiparity • denervation of pelvic floor (compression/traction injury to pudendal)
Iatrogenic • iatrogenic injury following: • lateral internal sphincterotomy • fistulotomy (reported as high as 35-45%) • hemorrhoidectomy • radiation therapy
Congenital malformations • spina bifida • imperforate anus • myelomeningocele • related to dysfunction of pelvic floor as well as abnormal proprioception of rectum
Diagnosis • history (obstetrical/ surgical), changes in bowel consistency, passive vs urge incontinence • quantify degree of incontinence • Cleveland Clinic Florida Fecal Incontinence Score (CCF-FIS)
CC Fecal Incontinence Scoring • 0 = perfect continence • 20= complete continence • never = 0, • rarely = <1x/month, • sometimes = >1x/month • usually = >1x/wk, • always = >1x/day
Diagnosis • physical examination: evidence of trauma, skin excoriation, fistulae, protruding hemorrhoids • inspect perineal body • patulous anus - check for prolapse
Diagnostic Studies • endoanal ultrasound - diagnostic cornerstone • internal sphincter - hypoechoic • external sphincter - hyperechoic • scar tissue - mixed echogenicity • measure perineal body thickness (PBT) - less than 10mm abnormal
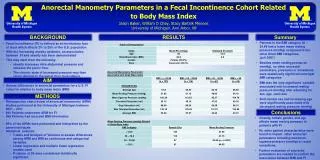
Diagnostic Studies • Anorectal manometry - functional status of anal sphincters and distal rectum • station pull through or continuous pull through • measurements: resting pressure (IAS), squeeze pressure (2-3x baseline), high-pressure zone (length of IAS, in women 2-3cm), RAIR (rectoanal inhibitory reflex), rectal sensation and compliance • RAIR - IAS relaxation with EAS contraction with small volume rectal distention - enables sampling reflex • absent in Hirschsprungs, Chagas, dermatomyositis, scleroderma
Diagnostic Studies • pudendal nerve terminal motor latency - electical impulses to PN with time response of EAS - nml 2.0 +/- 0.2ms • pudendal neuropathy implicated in poor outcomes p sphincteroplasty • EMG • defecography • colonoscopy
Nonoperative Management • medical therapy • biofeedback • secca procedure • injectables
Medical Therapy • bulking agents, constipating agents (lomotil, codeine, amytriptyline), laxative regimens with scheduled disimpaction (for overflow incontinence) • loperamide - synthetic opiod, inhibits small and large intesting Mu receptor - also increases IAS resting pressure, rectal sensation and increase RAIR
Biofeedback • pioneered in 1974 (Miller-Abbot balloon used as sensor to improve quality of Kegel exercises) • published studies with improvement of continence in adults and children with biofeedback 70% of time • long-term benefit less clear • randomized controlled trial (Heyman et al.) with pelvic floor exercise vs manometric biofeedback with 44% vs 21% able to achieve complete continence
Secca Procedure • high-frequency alternating current - modification of treatment for GERD • thermal energy - build collagen, shorten/remodel muscle • RF delivered 90s each quadrant at 5mm increments (usually 16-20 increments) • Takashi et al. 19 pts at 5 yr follow-up, in 16 pts >50% improvement
Injectables • developed from treatment of urinary incontinence with injectable bulking agent • safe, minimally invasive, outpatient administration • silicone vs carbon-coated microbeads • maximum improvement 1-6 mos, durability 1-2 yrs
Operative Treatment • overlapping sphincteroplasty • parks posterior anal repair • sacral nerve stimulation • artificial bowel sphincter • muscle transposition • fecal diversion
Anterior Overlapping Spincteroplasty • Anterior Overlapping sphincteroplasty - mainstay treatment for incontinence with ext sphincter defect • identification of ends with mobilization • levator plication at proximal extent of dissection • overlapping repair shown to be superior to end-to-end repair, though might be associated with evacuation difficulties • both with diminishing efficacy over time
Parks Posterior Anal Repair • treatment of neurogenic fecal incontinence - lengthen the canal and correct anorectal angle • curved incision behind anus, dissection in interspincteric plane • plicate pubococcygeus and puborectalis • published poor long-term results - 33% at 5 yrs
Sacral Nerve Stimulation • developed for urinary incontinence • staged procedure - percutaneous nerve evaluation (2wks), pts with improvement 50% or greater offered permanent stimulator • test stimulate S2, S3,S4 - goal is S3 stimulation to contract levator ani, external anal sphincter, plantar flexion of first 2 toes • complications rare - lead migration, infection, pain
Sacral Nerve Stimulation • largest prospective randomized trial with SNS - 16 centers, 120 pts with permanent stimulator placed • persistent benefit (50% reduction of symptoms) seen in 70% of pts at 36 mos f/u • interval measurements with 80% success
Artificial Bowel Sphincter • first reported in 1987 • transverse perineal incision with subcutaneous tunneling around anal canal • reservoir in space of retzius, pump in labia or scrotum, subcutaneous catheter • pump to evacuate - fluid goes from cuff to reservoir - passively refills
Artificial Bowel Sphincter • multicenter trial (2002) - 112 pts, 384 device-related complications in 99 pts • 25% infection • 46 revision rate • 85% pts reports successful outcome
Gracilis Muscle Transposition • first reported in 1952 for children with fecal incontinence 2/2 neurologic and congenital anomalies • mobilization of gracilis muscle with transposition of muscle around anal canal and fixation to the contralateral ischial tuberosity • poorer outcomes with h/o refractory diarrhea or constipation, obstetric injury, adv age • functionally pts can only control solid stool • skeletal muscle transposition - more easily fatigued
Gracilis Muscle Transposition • complications: evacuatory dysfunction, perineal pain, infection • stimulated gracilopasty with lead placement migration/erosion/infection, nerve fibrosis
Fecal Diversion • creation of colostomy or ileostomy if all measure fail • uncontrolled perineal stoma --> controlled abdominal stoma • majority of pts best-served with end-sigmoidoscopy • pts with slow transit or chronic constipation may be better served with ileostomy
Conclusion • fecal incontinence is a socially devasting condition and a symptom describing many etiologies • based on these etiologies, there are many non-operative and operative methods of improving quality of life