Download
1 / 18
180 likes | 321 Vues
Migrants, ethnic minorities, drug use and HIV. Lucas Wiessing, EMCDDA, Lisbon, 7 June 2007. < 5%. 5% or higher. not available. HIV prevalence among IDUs in the EU, samples with national and sub-national coverage 2004-2005. Notes: Data in [brackets] are sub-national

E N D
Migrants, ethnic minorities, drug use and HIV Lucas Wiessing, EMCDDA, Lisbon, 7 June 2007
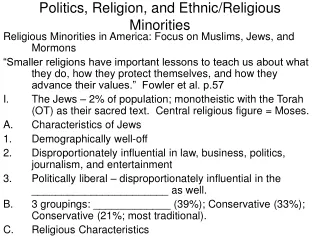
< 5% 5% or higher not available HIV prevalence among IDUs in the EU, samples with national and sub-national coverage 2004-2005 Notes: Data in [brackets] are sub-national Colour indicates midpoint of national data or if not available sub-national data Data Ireland 2003; Latvia 2003; Slovakia 2003-0 and from 2006 in case of Spain and Sweden
HIV prevalence among injecting drug users –national and subnational studies 2004-2005
HIV prevalence in samples of IDUs (‘all’) and in the subgroup of IDUs under age 25 (‘young’)
Some questions • Are IDUs among migrants or ethnic minorities at higher risk than other IDUs? • What is the impact of migration on the IDU - HIV epidemics in the EU? • Do migrants or ethnic minorities have equal access to prevention and treatment? • Should we collect data on migrant/ethnic status of IDUs? And if yes how?
‘Social exclusion, drugs and minorities in the EU’ (EMCDDA 2000) • Assimilated minorities • ‘Nomadic’ minorities • Jewish communities • ‘Visible’ minorities • Recent arrivals -> much heterogeneity
Ethnic minorities and drug use (EMCDDA 2007) • Most studies show similar or lower levels of drug use • A larger gender gap, particularly for non-Western migrants • However, greater risk of developing drug use problems (McCambridge and Strang 2005) • In turn, drug problems can reinforce social exclusion • Sometimes different patterns of drug use, e.g. khat among Somalians in England and northern Europe and the aversion to injection among Surinamese in the Netherlands (EMCDDA 2002; EMCDDA 2001).
Roma and HIV risks • Two studies in Spain (prisoners, IDUs -1995) showed a significantly lower seroprevalence of HIV among Roma than non-Roma inmates [data refer to periods 1990-1995 and 1995 respectively, both in Spain: Martin-Sanchez V, 1997; Martin V, 1998; citation in Hajioff S & McKee M 2000] • Among 324 men in a Roma community in Sofia, Bulgaria, 72% had had anal sex with women and 10% with men in the past 3 months, frequently unprotected; 16% reported selling sex and 32% paying someone for sex [Kabakchieva E et al. 2002; cited in Hamers F et al. 2006.]
Discrimination from within: nine qualitative interviews with Bengali women in drug treatment, London • Bengali female drug users are a hidden population engaging in high-risk behaviours, especially unsafe sex • Shame about drug use, antipathy towards injecting and stigmatization of drug use • Gender role expectations are strong and they face greater gender discrimination from within their community regarding drug use than their counterpart males • They experience profound barriers to treatment, which prevent them from accessing services at an earlier stage in their drug use [Cottew & Oyefeso, 2005]
EuroHIV – ‘Country of origin’ of HIV+ IDUs • Data for 2005 from 15 EU countries (54%) • 1462 IDU cases, 204 with different country of origin (12%) • 64 of the 204 come from ‘the West’ (WHO region), 65 come from ‘the East’, 8 from ‘the Centre’, thus the majority migrated within the European region • High proportions of ‘HIV+ IDU from other country of origin’ are found in countries with low rates of HIV in IDUs • Caution in interpretation: Country of birth, nationality, country of probable infection… many missing data Source EuroHIV
HIV-IDU cases reported in 2005 in EU countries where data are available on ‘country of origin’ Source: EuroHIVNote: Lux excluded
HIV in IDUs in low prevalence EU countries • Czech Republic: currently finding very high prevalence among Russian speaking IDUs • Slovak Republic: only 5 IDU cases to date, however most were likely infected abroad [L. Okruhlica pers. comm. 2007] • UK: HIV in IDUs perhaps increasing? large proportion of imported cases (from southern Europe) • Estonia was low prevalence country for IDUs up to 2000, then explosive spread among Russian speaking IDUsEstonia had no harm reduction measures in place…
Molecular typing of HIV in IDUs: Estonia, Northwestern Russia • Estonian outbreak caused by simultaneous introduction of two strains, one subtype A very similar to Eastern European strain (~8% of cases) and another similar to African strains (77%). Small variability in Estonia suggests point source introductions [Zetterberg et al. 2004] • HIV in IDUs in Northwestern Russia closely linked to other Russian IDU epidemics [Smolskaya etal. 2006]
Access to health care • Disparities in HIV-related mortality due to lower access to HAART of people with lower socio-economic status, female gender, ethnic minorities, and IDUs [Wood E et al. 2003] • Education and health literacy are important factors in HIV-treatment adherence and access to medical care [Kalichman 1999] • Likely also: insurance, legal status of migrants
Discussion • Is it useful to distinguish people by ethnicity, migrant status? This will depend on activity, policy in question • If intended to improve situation, probably yes • But, policies and attitudes to migrants can change from positive to negative • Country of birth, nationality, perhaps less sensitive • Ethnicity, race, religion… perhaps better collect unlinked and anonymously
Need to know at national level: • Are migrants / ethnic minorities at higher risk of specific health problems (IDU, HIV, other)? • Are the standard data collection systems sensitive enough to provide reliable data? • Is there a need for additional targeted (ethnographic) studies, prevention or treatment programmes, other services?
Conclusions • Data lacking and defining these groups is difficult • Drug use in migrants not necessarily higher • Immigration of HIV+ IDUs may have significant impact, but only on low level epidemics, and outbreak risk depends on prevention coverage • Access to services generally lower? (few data) • Collect sensitive data unlinked & anonymous and combine with repeated (ethnographic) surveys
Acknowledgements • Anthony Nardone, EuroHIV • Valerie Delpeche • Linda Montanari • Lubomir Okruhlica