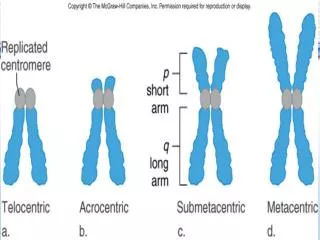
nt and aneuploidy
nt and aneuploidy. . Monosomics for all human autosomes die in utero. A sex-chromosome monosomic complement of 44 autosomes + 1 X produces the phenotype of Turner syndrome.

nt and aneuploidy
E N D
Presentation Transcript
. Monosomics for all human autosomes die in utero. A sex-chromosome monosomic complement of 44 autosomes + 1 X produces the phenotype of Turner syndrome. The most common type of viable human aneuploid is Down syndrome occurring at a frequency of about 0.15 percent of all live births The only other human autosomal trisomy to survive to birth are afflicted with either trisomy 13 (Patau syndrome) or trisomy 18(Edwards syndrome). Trisomies chromosome 2, 16, and 22 are relatively common in abortuses but never survive to birth. Trisomy of the sex chromosomes is possible, such as in (47,XXX), (47,XXY), and (47,XYY).
NT - MOST ROBUST MARKER • NASAL BONE • TRICUSPID FLOW • DUCTUS VENOSUS FLOW Usg markers
COMBINEDSCREENING MA+NT+BIOCHEMICAL MARKERS Advantages compared to second trimester biochemical screening include: Earlier diagnosis (11-14 weeks) Higher detection rates for fetal Down syndrome (80-90% or perhaps even higher compared to 75% for the second trimester "quad" screen and 60-70% for the older "triple" screen) Detection of most major chromosome abnormalities other than trisomy 21 Acts as a nonspecific marker for other birth defects including some major cardiac defects and syndromic conditions Can detect a number of major structural birth defects associated with normal chromosomes The primary disadvantage is Narrow window of entry (11-14 weeks with ideal entry at 11-12 weeks). WHY FIRST TRIMESTER
MATERNAL AGE + NT M A + NT + BIOCHEMICAL MARKERS M A + NT + B M + NB/DV FLOW/TCV FLOW. RISK 1 TO 50 NB –N NO CHANGE IN RISK RISK UPTO 1 TO 1000 NB- N RISK REDUCED NB-AB RISK INCREASED HYPOPLASTIC NB ALL OTHER MARKERS N –REPEAT SCAN REVERSE a WAVE RISK ALWAYS INCREASED NT AND ANEUPLODY
INCREASED NT A/W INCREASED FETAL MORTALITY INCREASED NT A/W STRUCTURAL ABNORMALITIES MAJOR CARDIAC DEFECTS DIAPHRAGMATIC HERNIA EXOMPHALOS SKELETAL DEFECTS BODY STALK ANOMALIES NT AND EUPLOID FETUS
I Fetal abnormalities The 11-14 week scan
Normally nuchal translucency disappears by 14 weeks. Noteworthy are cases with abnormal NT that resolve spontaneously around 14 weeks and show healthy outcome Chromosomally and structurally normal fetuses with history of thickened NT with no evidence of nuchal fold thickening or non-immune hydrops, at 20 weeks -- no increased risk for perinatal or long-term morbidity and mortality ABNORMAL NT NORMAL FETUS
Chromosomally and structurally normal fetuses with • Altered dermal collagen composition (eg, Down syndrome) • Abnormal nuchal lymphogenesis (eg, Turner syndrome) • Hemodynamic alterations and cardiac dysfunction( heartdefects) • Abnormal endothelial cell differentiation Pathophsiology of NT-
ABSENT PRESENT Nasal bone
NORMAL REDUCED INCREASED TRISOMY 21 MAXILLO FACIAL ANGLE
reverse a wave a/w chromosomal defects cardiac defects and adverse fetal outcome DUCTUS VENOSUS FLOW
Prevalence of TCV regurgitation in fetuses with trisomy 21 is about 74% whereas only 7% of chromosomally normal fetuses have this finding There is an increased prevalence of cardiac defects with TC regurgitation, irrespective of the presence or absence of aneuploidy Tricuspid flow
FETAL GROWTH/ CRL - REDUCED GROWTH CAN BE SEEN IN TRISOMY 13 ,18, TURNERS SYNDROME HOWEVER NOT IN TRISOMY 21 FETAL HEART RATE -BRADYCARDIA SEEN IN TRISOMY 18 AND TRIPLOIDY AND TACYCARDIA IN TRISOMY 13 AND TURNER SYNDROME FETAL MEASUREMENTS AS MARKERs
SINGLE UMBILICAL ARTERY/ TWO VESSEL CORD SEVEN FOLD INCRESED RISK FOR TRISOMY 18 FETAL STRUCTURAL DEFECTS AS MARKERS
MEGACYSTIS LONG. BLADDER OF >7MM 7-15 MM A/W INCREASED RISK OF TRISOMY 13 AND 18 EUPLOID FETUSES –SPONTANEOUS RESOLUTION >15 MM LESS LIKELY CHROMOSOMAL ANOMALIES MORE LIKELY TO CAUSE OBSTRUTIVE UROPATHY megacystis
HIGH ASSOCIATION WITH TRISOMY 18 ONE OF THE REASONS TO PERFORM NT SCREENING AT 11WEEKS NO PHSIOLOGICAL BOWEL HERNIATION OMPHALOCOELES WITH ONLY BOWEL HERNIATION STRONGER ASSO. WITH ANEUPLOIDY Aneuploid fetuses with omphalocoeles containing only bowel show resolution in significant no of fetuses, most likely developmental delay. OMPHALOCOELE
EXTREME FORM ALOBAR HOLOPROSENCEPHALY CAN BE DETECTED IN FIRST TRIMESTER INCREASED RISK OF ANEUPLOIDY MOSTLY TRISOMY 13 HOLOPROSENCEPHALY
THE FIRST TRIMESTER SCAN IS NO LONGER A NT SCAN BUT A FETAL ANATOMY SCAN The first trimester anomaly scan detectable abnormalities
INTRACRANIALTRANSLUCENCYIN OPEN NEURAL TUBE DEFECTS The fourth ventricle presents as an intracranial translucency (IT) between the brain stem and the choroid plexus. a case of open spinabifid demonstrating compression of the fourth ventricle with no visible translucency.
Arnold chiari 2 Lemon sign: Scalloping of frontal bones Banana sign: Caudal displacement of cerebellum , obliteration of CM Not consistently seen in first trimester.
NORMAL POST FOSSA CYST OPEN SPINA B Posterior fossa at 11 to 13.6 weeks
Meningoenc • Occipital (MC) – A/w skull defect (cf D/D Nuchal cystic hygrom • ParietalFrontoethmoidal A/w Microcephaly, Hydrocephalus, Spina bifida, Meckel Gruber Syn. Neural Tube Defects d/d : Cystic Hygroma
SKULL OSSIFICATION AT 11 WEEKS OF OCCIPITAL BONE Varying degrees of distortion of brain ACRANIA–exencephaly-Anencephaly
Encephalocoele Polycystic kidneys Polydactyly MeckelGruber Syndrome
Complete or partial absence of cerebellar vermis 4th Ventricle Dilatation End point of chromosomal abn. , Genetic Syndromes , congenital infection or Isolated abn DANDY WALKER COMPLEX
Total absence of cerebral hemispheres • Large head • Small hemispheres • Fluid-filled intracranial cavity with no midline echoes Hydranencephaly
Alobar and Semilobara/w facial abnormalities Lobar Holoprosencephaly
Rare Cervical dysraphism with occipital(inion) defect +encephalocoele Persistently extended fetal head -clue Iniencephaly
Fetal 4 chamber view can be demonstrated at 11to 14 weeks scan RAISED NT PERSISTENT BRADYCARDIA (60BPM) COMPLETE AV CANAL DEFECT A 14 WEEK SPECIALIST SCAN CAN REVEAL MAJOR ABN OR RAISE SUSPICION FOR LATER DETAILED SCAN Cardiac anomalies
AV CANAL DEFECTS VSD 4 CHAMBER VIEW
CAUDAL REGRESSION SYNDROME DEGREES OF VERTEBRAL ANOMALIES FROM PERTIAL SACRAL AGENESIS TO ABCENCE OF LUMBAR SPINE. 250 TIMES MORE COMMON IN POORLY CONTROLLED DIABETIC MOTHERS ABSENT LIMBS MUSCULOSKELETAL ABN.
PHSIOLOGIC BOWEL HERNIATION AT 9 TO 11 WEEKS EXOMPHALOS - a/w CHROMOSOMAL DEFECTS .CORD INSERTION AT APEX OF SAC VS GASTROCHISIS PARA MIDLINE HERNIA SAC BODY WALL ANOMALIES
PYELECTASIS RANGE MEGACYSTIS CYSTIC DYSPLASTIC KIDNEY RENAL AGENESIS POLYCYSTIC KIDNEYS URINARY ANOMALIES
Fetal cardiac examinations optimally performed between 18-22 weeks. Some anomalies may be identified in late first and early second trimester especially when increased nuchal translucency is identified. 4 chamber view, 3 vessel view and outflow tracts can detect 80% -85% of cardiac anomalies CARDIOVASCULAR ANOMALY
BASIC VIEW four chamber view
EXTENDED BASIC VIEWS Left ventricular outflow tract(LVOT) Right ventricular outflow tract(RVOT)
One of the most common congenital cardiac anomaly VSD is easily diagnosed on the four-chamber view alone. However, color Doppler US may be needed to demonstrate smaller defects and some may not be detected until after birth. Small VSD (MUSCULAR)show spontaneous closure VSD
When the endocardial cushions fail to fuse, a wide range of atrioventricularseptal defects occur. ENDOCARDIAL CUSHION DEFECT (four-chamber view) shows absence of the interventricular and interatrial septa, thus producing connections between the ventricles and between the atria.
The undivided truncus receives blood from both ventricles. A VSD is almost always present PERSISTENT TRUNCUS ARTERIOSUS a.(four-chamber view) shows a VSD (arrow). Dao descending aorta. b.(base view) shows a single trunk (arrow) overriding both ventricles.
Small left ventricle, which is associated with aortic atresia. Atretic or hypoplastic mitral valve. HYPOLPASTIC LEFT HEART SYNDROME Hypoplastic left heart syndrome in a fetus (four-chamber view) shows that the left ventricle is small relative to the right ventricle and the left atrium is small relative to the right atrium.
CAUDALLY PLACED TRICUSPID VALVE /OFFSET BETWEEN MITRAL AND TRICUSPID VALVE /ENLARGED RT VENTRICLE /TRICUSPID REGURGITATION EBSTEIN ANOMALY
PARALLEL OUTFLOW TRACTS , LARGE RT VENTRICLE ,SMALL LT VENTRICLE DOUBLE OUTLET RIGHT VENTRICLE
NORMAL HEART RATE 2ND IS 120BPM TO 160BPM FETAL ARRYTHMIAS can now be defined precisely for mechanism-specific therapy and for subsequent monitoring of response. RHYTHM AMNORMALITIES OF HEART
FETAL SKELETAL STRUCTURES TO BE SEEN: FETAL CRANIUM(BPD, HC) ABDOMINAL CIRCUMFERENCE(AC) MANDIBLE CLAVICLE SCAPULA CHEST CIRCUMFERENCE ALL FETAL LONG BONES( RHIZOMELIA, MESOMELIA, MICROMELIA) FETAL FACIAL PROFILE(GLABELLAR BOSSING, FLATTENED NASAL BRIDGE, MICROGNATHIA) VERTEBRAL BODIES HAND AND FEET( EXTRA/MISSING/MALFORMED DIGITS) MINERALISATION PATTERN. CHEST:ABDOMEN CIRCUMFERENCE( <0.6 ABNORMAL) FL:AC RATIO(<0.16 ABNORMAL) FL: FOOT LENGTH RATIO(<1 ABNORMAL) MSK ANOMALIES
FETAL LONG BONES: PRESENCE/CURVATURE/MINERALISATION/FRACTURES The femur length–abdominal circumference ratio (<0.16 suggests lung hypoplasia) femur length–foot length ratio(normal = 1, <1 suggests skeletal dysplasia) THORAX: CHEST CIRCUMFERENCE/ CT RATIO MEASURED AT THE LEVEL OF FOUR CHAMBER VIEW OF HEART. HAND AND FEET: PRE AND POSTAXIAL POLYDACTYLY/SYNDACTYLY/CLINODACTYLY/OTHER DEFORMITIES SKULL:HC/BPD/SHAPE/MINERALISATION/OSSIFICATION. FACIAL STRUCTURES:MICROGNATHIA/ SHORT UPPER LIP/ABNORMALLY SHAPED EAR/FRONTAL BOSSING/CLOVERLEAF SKULL. PELVIS: HYPOPLASTIC ACETABULAE/FLAT ILIAC BONES. CONTD..
LIMB DEFICIENCY: complete absence –amelia, incomplete absence-meromelia. FETAL SKELETAL DYSPLASIA lack of a normal hand and the abnormal soft tissue at the distal end of the forearm
Disproportionate dwarfism with very short extremities,which are bowed in type 1 and may be straight in type 2. Thorax is narrow. Cloverleaf skull deformity is generally seen in type 2. Polyhydramnios is present in almost 50% of cases. Pulmonary hypoplasia. THANATOPHORIC DYSPLASIA telephone receiver–shaped femur hypoplastic thorax