Download
1 / 40
400 likes | 836 Vues
PCMH and Health Coaching. April 2014. Provide an overview of Patient Centered Medical Home, Population Health Management and the role of the Health Coach in PCMH, Population Health initiatives and working with individual clients. Purpose.

E N D
PCMH and Health Coaching April 2014
Provide an overview of Patient Centered Medical Home, Population Health Management and the role of the Health Coach in PCMH, Population Health initiatives and working with individual clients. Purpose
Identify two components of a Patient Centered Medical Home • Describe two ways a Health Coaching interaction differs from a typical patient/staff interaction • Identify one action you can take to help improve the health of your patients that contributes to Population Health Management Objectives
Show of hands • Who works in a clinic that has attained Patient Centered Medical Home designation? • What factors drove this change? Poll Question
Enhanced patient experience of care • Improved quality • Improved efficiency Triple Aim
Demonstrates that you and your colleagues put the patient at the center of care • Continuity of care • Quality • Patient Safety • Enhanced reimbursement for clinic • Relationship building with patient and team • Improved quality of work life Why become a PCMH?
Enhanced Access and Continuity • Identify and Manage Patient Populations • Plan and Manage Care • Provide Self-Care and Community Support • Track and Coordinate Care • Measure and Improve Performance NCQA 2011 Standards for PCMH Recognition
Patient-Centered Access • Team-Based Care • Population Health Management • Care Management and Support • Care Coordination and Care Transitions • Performance Measurement and Quality Improvement NCQA 2014 Standards for PCMH Recognition
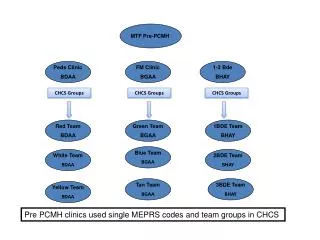
Focus on Population Health in Diabetes • Wagner’s Chronic Care Model • Data driven • Implementation of Registries and EHR • NCQA Diabetes Recognition for providers • Health Coaching Our path to PCMH
3% of population 39% of cost Population Health Management 40% of population 41% of cost 50% of population 7% of cost Slide provided by the Clinical Health Coach Training Program
Social • Emotional • Economic • Physical Cost of Chronic Disease
The coordination of care delivery across a population to improve clinical and financial outcomes, through disease management, case management and demand management. Population Health Management
In 2000 MMS implemented the Improving Diabetes Outcomes project in 13 clinics • Wagner’s Chronic Care Model MMS path to Population Management in Diabetes
ADA Standards of Care for Diabetes • A1c in past 12 months and value • LDL in past 12 months and value • Microalbumin in past 12 months • BP < 130/80 • Dilated Retinal Exam in past 12 months • Monofilament foot exam in past 12 months MMS path to Population Management in Diabetes
The Dual Challenge of Diabetes and Hypertension project • Diabetes Recognition Program • Wellmark Collaboration on Quality • Health Coaching • PCMH • IME Health Home MMS path to Population Management in Diabetes
Data • Excel spreadsheet initially • CDEMS Registry (free download) • Wellcentive Registry • Implementation of Electronic Health Record • Currently building reports that will allow us to query EHR MMS path to Population Management in Diabetes
National Quality Forum http://www.qualityforum.org • US Preventive Services Task Force http://www.uspreventiveservicestaskforce.org/recommendations.htm Best Practice Guidelines
NCQA http://www.ncqa.org • Diabetes Recognition Program • Heart/Stroke Recognition Program • PCMH Recognition Best Practice Guidelines
In 2000 it was the right thing to do • No monetary incentive • Possible negative financial impact in FFS environment • Pay for Performance programs • Insurance companies – quality and cost containment Driving Forces: Past
Patient Centered Medical Home Recognition • Financial benefit to clinics • Affordable Care Act • CMS’ move to Value Based instead of Fee for Service Payment • No payment for readmission in 30 days • ACO Driving Forces: Present & Future
Ruby Slipper Moment • The moment the patient recognizes that the power to make the changes lies within.
The Ineffective Physician: Non-Motivational Approach - YouTube www.youtube.com/watch?v=80XyNE89eCs • The Effective Physician https://www.youtube.com/watch?v=URiKA7CKtfc Video Examples
Structuring the interaction using OARS+E • Open ended questions • Affirmation • Reflection • Summarizing • Eliciting Change Talk Motivational Interviewing - OARS+E
Why • Am • I • Talking Health Coaching - WAIT
We automatically want to fix things • Advice giving • Directing the patient • You should …. conversations • Not recognizing the person’s power to make change from within Health Coaching - Righting Reflex
“I knew I needed to fulfill a previously set goal of walking 30 minutes a day but I easily made excuses and put off walking…….Carol and I talked about it. She didn’t tell me that I had to walk for exercise. She said just enough to make me want to do it. That motivated me to become more disciplined…Now that I have established the habit with Carol’s coaching, walking has become a pleasure that I look forward to.” • A1c improved from 7.4 to 7.1 in 6 months with the walking program Patient Quote
Credible data is imperative to success • Front end functions must be done well to submit a successful application • Eg. 50% of all patients who request an electronic copy of their health information must be provided it within 3 business days • Electronic system with functionality a must have A NCQA PCMH Experience
Coordinating care across the continuum • Must support patients and demonstrate this is done • Provide input to key brochures • Patient access key • Application requires extreme attention to detail • Do not hesitate to contact reviewer with questions A NCQA PCMH Experience
Your work benefits your patients, coworkers and the clinic’s bottom line • Be prepared for change • Be willing to stretch • New processes and workflows • Work to the top of your licensure • Leverage technology Youmatter in the PCMH
Care delivery in a PCMH is a TEAM EFFORT • Huddle Video link PCMH TEAM
Enhance Access and Continuity • Chart Scrub • Pre-visit Planning • Run daily huddle • Identify and Manage Patient Populations • CMA roles vary - some are in data analysis roles in a clinic How do I contribute to PCMH?
Plan and Manage Care: • Pre-visit Chart review: • Identifying gaps in care • Addressing those gaps contributes to improving the health of individual patients and the entire patient population How do I contribute to PCMH?
Provide Self-Care and Community Support • Look for the patient’s strengths and capitalize on those strengths • Utilize patient education materials • Link patient to community resources How do I contribute to PCMH?
Track and Coordinate Care • Referral Tracking System • Measure and Improve Performance • Utilize Clinical Guidelines in your daily work • Utilize data to improve care How do I contribute to PCMH?
Contact Information: Carol Brinkert RN, BAN, CHC brinkerc@mercyhealth.com Danielle Pingel, MHA danielle.lentsch@mercyhealth.com Thank You