ASCOT TRIAL
ASCOT TRIAL. Abbas Zaidi 20/09/05. Hypertension is one of the most prevalent risk factors for cardiovascular disease, affecting as many as 800 million people worldwide.

ASCOT TRIAL
E N D
Presentation Transcript
ASCOT TRIAL Abbas Zaidi 20/09/05
Hypertension is one of the most prevalent risk factors for cardiovascular disease, affecting as many as 800 million people worldwide. • It is estimated that at least 80 percent of people with high blood pressure may also have other uncontrolled cardiovascular risk factors with elevated cholesterol being the most common.
In a typical Western country with a population of 50 million people, about eight million receive treatment for high blood pressure; beta-blockers and diuretics.
The NICE guideline advises that first-line treatmentshould be • A low-dose thiazide diuretic • Except inpatients under 55 with moderately raised blood • pressure, for whom a beta-blocker may be moreeffective and should be considered as an alternativefirst-line therapy. • If monotherapy is unsuccessful, a beta-blocker shouldbe added. • The combination of a thiazide and a beta-blocker may still be effective in patients under 55 butis associated with a slightly increased risk of diabetes.
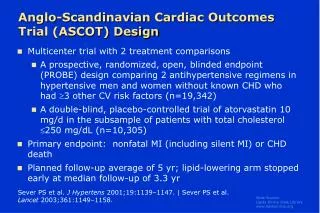
Introduction • Several randomized clinical trials in hypertension have documented that most of the antihypertensive drug classes reduce major cardiovascular end points such as heart attack, stroke, and congestive heart failure to a similar extent. Therefore, most authoritative guidelines have time and again recommended to preferentially use b-blockers and diuretics because they are less expensive than the newer drugs, such as calcium antagonists and blockers of the renin-angiotensin system (ARBs). • The rationale for the design of the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT) was the lack of outcome data for the two most commonly used newer drug classes--that is, calcium antagonists and ACE inhibitors, and to compare this combination with a b-blocker/diuretic combination.
Aim • The primary objective of ASCOT was to compare the long-term effect on non-fatal myocardial infarction (MI) and fatal coronary heart disease of a standard antihypertensive regimen (b-blockers and diuretic) with a more contemporary combination of a calcium antagonist blocker and an ACE inhibitor.
It was conducted in more than 650 general practices and 32 regional medical centers across the United Kingdom, Ireland, and the 5 Scandinavian countries (Denmark, Finland, Iceland, Norway, and Sweden).
The ASCOT results predicted that, if the amlodipine and perindopril combination were prescribedin only half of the patients currently receiving a beta-blocker/diuretic combination for the treatment of high blood pressure, over a 5 1/2 year period • There would be nearly 100 000 fewer cardiovascular events and procedures, nearly 40 000 fewer strokes and 35 000 fewer deaths from cardiovascular disease. There would also be over 90 000 fewer patients who develop type 2 diabetes.
Method:ASCOT was an independent, multicenter, randomized study designed to evaluate the separate and combined effects of antihypertensive and lipid-lowering therapy on cardiac outcome in patients (n = 19,342) with hypertension and no history of coronary heart disease. • The study used a prospective, randomized, open, blinded end point (PROBE) design to compare the effects of a calcium antagonist-based regimen (amlodipine) plus an ACE inhibitor (perindopril, if necessary) versus a b-blocker-based regimen (atenolol) (plus a diuretic, bendroflumethiazide-K, if necessary).
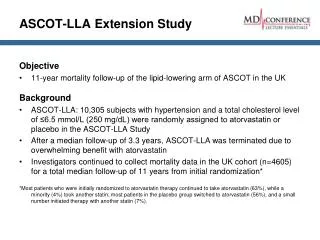
ASCOT LLA • A subset of patients were further randomized to receive atorvastatin 10 mg/d (n = 5168) or placebo (n = 5137) in a double-blind fashion.
The trial protocol called for bringing nondiabetic patients to blood pressure targets of < 140 mm Hg systolic blood pressure and < 90 mm Hg diastolic blood pressure • Diabetic patients to targets of < 130 mm Hg SBP and < 80 mm Hg DBP.
The 2 antihypertensive regimens were administered in 6 incremental steps, depending on whether patients achieved their blood pressure goals. First-line drugs were increasing doses of amlodipine or atenolol, followed by combination with perindopril or BFZ, respectively, to bring patients to goal. If this was not sufficient, the alpha-blocker, doxazosin could be added as a third drug, at the discretion of the physician, to either of the 2 drug combinations
Table 1. ASCOT-BPLA: Antihypertensive Regimens "Newer" Regimen "Standard" Regimen Step 1 Amlodipine 5 mg Atenolol 50 mg Step 2 Amlodipine 10 mg Atenolol 100 mg Step 3 Amlodipine 10 mg Atenolol 100 mg Perindopril 4 mg BFZ + K 1.25 mg Step 4 Amlodipine 10 mg Atenolol 100 mg Perindopril 8 mg BFZ + K 2.5 mg Step 5 Amlodipine 10 mg Atenolol 100 mg Perindopril 8 mg BFZ + K 2.5 mg Doxazosin GITS 4 mg Doxazosin GITS 4 mg Step 6 Amlodipine 10 mg Atenolol 100 mg Perindopril 8 mg BFZ + K 2.5 mg Doxazosin GITS 8 mg Doxazosin GITS 8 mg BFZ = bendroflumethiazide; GITS = gastrointestinal therapeutic system; K = potassium
In October 2004, the independent Data Safety Monitoring Board (DSMB) recommended stopping ASCOT due to benefits in favor of amlodipine/perindopril-based antihypertensive therapy compared with atenolol/bendroflumethiazide-K-based antihypertensive therapy. • . • The data safety monitoring board determined that there was a higher event rate in the atenolol arm.
Amlodipine/Perindopril Atenolol/BFZ Baseline Study end Baseline Study end SBP (mm Hg) 164.1 135.5 163.9 136.3 DBP (mm Hg) 94.8 71.1 94.5 78.4 Blood pressure was well controlled in both arms of the study (Table 2). At the end of the study, mean blood pressure was lower in the amlodipine/perindopril group by 2.9/1.8 mm Hg. Table 2. ASCOT-BPLA: Mean Blood Pressure Over Time BFZ = bendroflumethiazide; DBP = diastolic blood pressure; SBP = systolic blood pressure
The combination reduced • Major cardiovascular events by 16% (P<0.001), • Stroke by 23% (P=0.003) • Cardiovascular mortality by 24% • Total mortality by 11% (P=0.025) compared with the regimen of the beta-blocker atenolol with or without bendroflumethiazide. • There were significantly fewer new cases of diabetes, 567 versus 799 (P<0.0001)
What Were the Reasons for These Results? • Several possible explanations for the results: • Better blood pressure lowering with amlodipine/perindopril • An adverse interaction between atenolol/thiazide and the statin • A beneficial interaction between atenolol/thiazide and the statin • Extra blood pressure-lowering benefits of amlodipine/perindopril; and • Non-blood pressure-lowering disadvantages for atenolol/thiazide.
The ASCOT researchers said that the blood pressure by itself can only explain 15% to 35% of the positive outcomes in the amlodepine arm.
Conclusion • The results of ASCOT are substantial and important. • We must consider whether the much-used regimen of beta-blockers followed by thiazides is the automatic choice for our patients.