ASCOT
ASCOT. ASCOT STUDY. ASCOT. INTRODUCTION AND AIMS EXISTING KNOWLEDGE BACKGROUND OF ASCOT STUDY DESIGN (TWO ARMS (BPLA,LLA) METHODOLOGY TREATMENT REGIMES USED IN ASCOT RESULTS (BPLA published in 4/9/05) CHANGE IN GUIDELINES ?? HOW DOES IT AFFECT GP’S ??.


ASCOT
E N D
Presentation Transcript
ASCOT ASCOT STUDY
ASCOT • INTRODUCTION AND AIMS • EXISTING KNOWLEDGE • BACKGROUND OF ASCOT • STUDY DESIGN (TWO ARMS (BPLA,LLA) • METHODOLOGY • TREATMENT REGIMES USED IN ASCOT • RESULTS (BPLA published in 4/9/05) • CHANGE IN GUIDELINES ?? • HOW DOES IT AFFECT GP’S ??
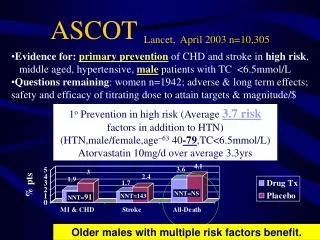
Largest study of high blood pressure treatment ever conducted in Europe. Results were published in the European Scoiety of cardiology in September 4th 2005. Combination of effective modern antihypertensives along with lipid lowering drugs can reduce the incidence of strokes CHD, cardiovascular deaths and prevent the onset of diabetes. INTRODUCTION
INTRODUCTION AND AIMS • Launched in 1997 & funded by Pfizer • Independent investigator led study • Designed to evaluate different treatment strategies for preventing cardiovascular disease in hypertensive patients. • Compare the effects of two treatment strategies on non fatal MI and fatal CHD.
EXISTING KNOWLEDGE • Hypertension is one of the most prevalent risk factors for cardiovascular disease, affecting 800 million people worldwide. • At least 80% of these would have other uncontrolled risk factors of which raised cholesterol is the commonest. • We all know that reduction of blood pressure is central to reducing mortality due to MI, CVA etc. • Traditionally beta blockers & diuretics are used to treat hypertension • Newer drugs like calcium channel blockers and ACE inhibitors are also used to treat hypertension.
BACKGROUND • Conducted in 650 practices and 32 regional medical centres in the UK, Ireland and the 5 Scandinavian countries.(Denmark, Norway, Sweden,Iceland and Finland) • The impetus of this study was lack of outcome data on the newer types of antihypertensives.
BACKGROUND contd • No evidence so far on the outcome of specific combination regimes in lowering blood pressure. • Evidence of shortfall in the prevention of CHD using standard therapies using beta blockers and diuretics. • Need to evaluate multiple risk factor intervention in the prevention of CHD. • Previous trials have shown that beta blockers and diuretics are better than hydrallazine and methyldopa.(these are no longer commonly used)
DESIGN • Multicentric international trial that involves two treatment comparisons in a factorial design. • A prospective, randomized open blinded ,end point design study (PROBE) comparing 2 antihypertensive regimens (BPLA) • A double blind, placebo controlled trial of a lipid lowering agent in a subsample of those hypertensive patients.(LLA)
METHODOLOGY • 19,257 patients in the age group of 40-79 years were recruited between 1998-2000. • Other eligibility criteria were • No contraindications to the drugs • Able to attend clinic regularly for 5 years • BP >160/100 untreated or >/= 140/90 treated. • No previous MI or CHD • 3 or more risk factors for cardio vascular event i.e. smoking, NIDDM, Male, age >55.
Treatment regimes BPLA • The trial protocol was to reduce the BP to 140/90 in non diabetic and to 130/80 for diabetics. • The 2 antihypertensive regimes were administered in 6 incremental steps, depending on whether patients achieved their goals. • First line drugs were amlodipine or atenolol, followed by combination with perindopril or bendrofluazide.
RESULTS • 9639 patients received Amlodipine/ Perindopril treatment regime. • 9618 patients received atenolol/ Bendrofluazide treatment regime. • 18% were already on Asprin • 10% were on lipid lowering drugs. • Median follow up was 5.4 years. • Only 14% of patients on the amlodipine group and 9% of patients on the atenolol group remained on monotherapy.
RESULTS contd. • Blood pressure was well controlled in both arms of the study, but lower in the amlodipine group. • Average BP before the study for the amlodipine group was 164.1/94.8, which was reduced to 135.5/71.1 after 5.4 years. • For the atenolol group blood pressure dropped from 163.9/94.5 to 136.3/78.4.
RESULTS contd. • 14% risk reduction in all cause mortality in the amlodipine group • 10% reduction in the primary endpoint of nonfatal MI or fatal CHD. • 23% reduction of fatal and non fatal stroke. • 24% reduction in cardiovascular mortality. • 16% reduction in total cardiovascular events and revascularisation procedures.
RESULTS contd. • 32% excess incidence of new onset diabetes on the atenolol group. • Reduction in the incidence of renal impairment • Reduction in the incidence of peripheral vascular disease.
Study was terminated after a median period of 3.3 years by the data and safety monitoring board as there was significant reduction in the primary endpoint as well as in the incidence of strokes. Total of 10,297 of the patients enrolled in the ASCOT were eligible for the lipid lowering arm of the study. RESULTS (LLA)
36% reduction in non fatal MI and fatal CHD. 27% reduction in fatal and non fatal stroke 41% reduction in chronic stable angina. 13% reduction in total mortality. 21% reduction in revascularisation procedures 29% reduction of total cardiac events. RESULTS LLA (contd)
CHANGES TO GUIDELINES?? • Professor Peter Littlejohns, NICE Clinical and Public Health Director, commented: • “NICE guidelines are not usually considered for updating until four years after publication. • However in this case, because a potentially significant piece of new evidence is about to be published, NICE feels it is appropriate to look at this data in the context of our existing recommendations to see whether any revision might be necessary.”
CONTD • Professor Bryan Williams, a member of the Guideline Development Group added: “Early indications from the ASCOT study suggest that the results have the potential to change the pharmacological treatment algorithms in the current NICE and BHS guidelines.
HOW DOES THIS AFFECT GP’S • Adds to the existing confusion. • BHS guidelines downgraded the use of beta blockers as first line treatment. • NICE still recommend beta blockers and thiazide as first choice. • ASCOT recommends amlodipine and perindopril. • Cost implications.