Download
1 / 8
91 likes | 277 Vues
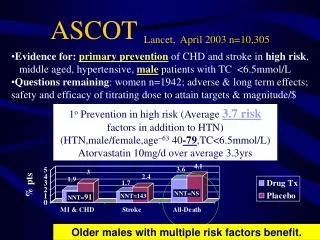
ASCOT Lancet, April 2003 n=10,305. Evidence for: primary prevention of CHD and stroke in high risk , middle aged, hypertensive, male patients with TC <6.5mmol/L Questions remaining : women n=1942; adverse & long term effects;

E N D
ASCOT Lancet,April 2003 n=10,305 • Evidence for:primary prevention of CHD and stroke in highrisk, • middle aged, hypertensive, male patients with TC <6.5mmol/L • Questions remaining: women n=1942; adverse & long term effects; • safety and efficacy of titrating dose to attain targets & magnitude/$ 1o Prevention in high risk (Average 3.7 risk factors in addition to HTN) (HTN,male/female,age~63 40-79,TC<6.5mmol/L) Atorvastatin 10mg/d over average 3.3yrs NNT=NS NNT=91 NNT=143 Older males with multiple risk factors benefit.
PROVE-ITNEJM,April, 2004 n=4,162 2yrs • Intensive vs moderate lipid lowering in high risk ACS pt • LDL: 2.74 baseline mmol/L 1.60atorv 80mg vs 2.46 pravastatin 40mg • 1o end point “Death or CV Event”: all-cause mortality, MI, unstable angina, revascularization, and stroke Mean age ~58 over 2years Atorvastatin 80mg/d $87 vs Pravastatin 40mg/d $42 After an Acute Coronary Syndrome (ACS) % patients NNT=NS NNT=26 (RRR=15%) NNH=46 Monitor for SE if using higher doses
TNTNEJM,April 2005 n=10,001 4.9yr • Intensive lipid lowering in stable CHD (n=15,464 - 8wk run-in) • LDL: 3.9 baseline mmol/L 2.0atorv80mg vs 2.6 atorv 10mg;Age 35-75, ~61 • 1o end point: “CHD Death, CV Event or Procedure, Stroke” • CV & Stroke events; NNT=46 / 4.9yr; • LFT's NNH=100; All-cause death5.7 vs 5.6% BUT non-CV death 3.2 vs 2.5 NS Atorvastatin 80mg/d $87 vs 10mg/day $67 % patients NNT=26 / 4.9yr (RRR=20%) NNT=NS LFTs 3xNNH=100 CV events; ADRs; NO difference in all-cause death
IDEALJAMA,Nov 2005 n=8888 4.8yr • Intensive lipid lowering in previous MI pts (open label trial) • LDL: 3.14 baseline mmol/L 2.1atorv80mg vs 2.7 simv 20-40mg;Age<80, ~62 • 1o Primary: Coronary Death, nonfatal MI or cardiac resusc.9.3 vs 10.4% NS • 2o Major vascular events (1o & stroke) NNT=59/4.8yr;MI6 vs 7.2% NNT=84 • LFT's NNH=112; All-cause death8.2 vs 8.4% or CV death5 vs4.9 butat least non-CV death 3.2 vs 3.5 NS Atorvastatin 80mg/d $87 vs Simv 20-40mg/day $41 % patients NNT=59 / 4.8yr (RRR=13%) NNT=NS LFTs 3xNNH=112 CV events; ADRs; NO difference in all-cause death
Highest risk benefit most! LDL Outcome Data
page 55 NNT based on risk
page 11 Statins best outcome evidenceAge up to age 80 (HPS) Low risk women no/? benefit 20 benefit a lot; 10 small benefit