High Frequency Ventilation
High Frequency Ventilation. Level 1 Mark Willing, RRT-NPS. Indications for High Frequency Ventilation. Failure of conventional mechanical ventilation to relieve respiratory acidosis

High Frequency Ventilation
E N D
Presentation Transcript
High Frequency Ventilation Level 1 Mark Willing, RRT-NPS
Indications for High Frequency Ventilation • Failure of conventional mechanical ventilation to relieve respiratory acidosis • Those patients at risk for or have developed a pneumothorax, pulmonary interstitial emphysema, pneumomediastinum, or other air-leak syndrome • A general “lung protective” ventilator strategy
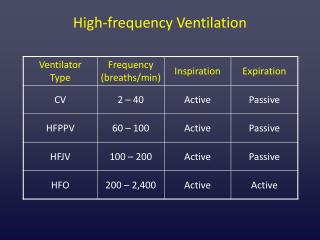
General Concepts • Low tidal volumes (less than 2ml/kg) • Rapid rates (up to 900 breaths/min) • May be “lung protective” due to decreased volutrauma • May be more efficient at ventilation than conventional ventilation methods
Enhanced Efficiency of Ventilation • Ventilationduring high frequency ventilation is achieved by a combination of factors contributing to enhanced removal of CO2 • Simultaneous inspiration and expiration due to unique gas flow pattern • Dependent upon maintaining as many open alveoli as possible • Enhanced mixing of gases in the airways and between alveoli
Gas entering the lungs travels centrally, while gas leaving the lungs swirls around it
Minute Ventilation • The amount of gas that is exchanged within the lung in one minute is called minute ventilation • As minute ventilation is increased, the amount of CO2 in the blood may decrease • Minute ventilation during conventional ventilation and spontaneous breathing is calculated as: • Respiratory Rate X Tidal Volume • Minute ventilation during high frequency ventilation is calculated as: • (Respiratory Rate)0.5 X (Tidal Volume)2 • Therefore, tidal volume is the primary determinant of minute ventilation during high frequency ventilation
High Frequency Jet Ventilation Concepts • The inhalation valve is placed as close to the patient as possible to deliver a “crisp” jet stream of fresh gas deep into the lungs. • A conventional ventilator is used in tandem to assist in oxygenation. Through manipulation of inspiratory time, PEEP, PIP, and rate, the mean airway pressure can be adjusted for optimal oxygenation and alveolar recruitment. • Passive exhalation requires a “lower” set rate (320-480 breaths/minute)
High Frequency Jet Ventilator Adjustments • Increasing the PIP setting may increase the delivered tidal volume, therefore lowering the CO2 in the blood…and vice-versa • Oxygenation is primarily influenced by the conventional ventilator through manipulation of the PEEP, PIP, inspiratory time, and rate
Servo Pressure • Respiratory therapists and nurses, alike, will be charting the servo pressure • Servo pressure is an indirect measurement of the delivered tidal volume • Changes in servo pressure give the bedside practitioner information regarding changes in compliance and resistance • As the servo pressure increases, it may be indicative of improving compliance and resistance…and vice-versa.
Common Alarms • “Cannot meet PIP” and/or “Loss of PIP” • Leaks in the circuit (associated with an acute increase in servo pressure and high servo alarm). Little or no chest wiggle and breath sounds. • Excessive respiratory effort by the patient (associated with repeated high/low servo and mean airway pressure alarms). • Recent disconnect for suctioning or repositioning (associated with a high/low servo and mean airway pressure alarm). • Near or complete extubation (associated with a high servo pressure and alarm). Loud upper airway noises, little to no chest wiggle, air escaping out the mouth.
What To Do • These two alarms are commonly associated with circuit disconnects and suctioning, which may be associated with severe, and perhaps life-threatening, alveolar collapse and oxygen desaturation. • The RN must notify the RRT and have this person available at the bedside prior to position changes, suctioning, and surfactant administration. • In the event that the RRT is currently unavailable, it is best to leave such “elective” procedures until such time an RRT can assist with or perform the procedure without the RN. • If at any other time, if the ventilator fails to establish the set PIP, immediately notify the respiratory therapist. • Hand-bagging a patient with a manual resuscitator bag may be very dangerous to certain premature infants, therefore immediate response from a respiratory therapist is critical.
Positioning the Circuit • The small bore, clear tubing coming off the jet adapter must not be in a dependent position. Any secretions or water obstructing the tube will result in inaccurate pressure readings, damage the pressure transducer in the patient box, and/or will cause inaccurate pressure delivery to the patient. • The elbow on the in-line suction catheter should be positioned in such a manner that water condensation is not injected or lavaged down the airway. • The green jet tubing should be as straight as possible to reduce any dampening of the jet stream into the airway.
High Frequency Oscillatory Ventilation Concepts • Open as many alveoli as possible without over distending the lung • May create blood pressure problems due to high lung volume, therefore volume expanders and/or vasoactive drugs may be needed • Active exhalation…pulls the gas out of the lungs on the expiratory cycle • Active exhalation allows for higher set ventilatory rates (up to 900 breaths/min)
The SensorMedics high frequency oscillator pushes and pulls gas above and below a set mean airway pressure
Settings • Frequency (Hertz, Hz) • Mean Airway Pressure (MAP) • Amplitude (Delta P, change in pressure)
Hertz (Hz) • 60 cycles in a minute = 1 Hertz • 120 breaths/min = 2 Hz, and so on • 15Hz on an oscillator is 900 breaths/min • The smaller the patient, the higher the Hz setting,…and vice-versa • Less than 2kg patient = 12-15Hz • Children in the PICU may be on 6-10Hz
Mean Airway Pressure (MAP) • Primary determinant of alveolar lung volume and critical to the efficiency of ventilation and oxygenation • Use chest X-rays to determine over/under-inflation of lung and then adjust MAP accordingly
Amplitude • Amplitude = Delta P = Change in pressure • As the change in pressure increases, it may increase the tidal volume, therefore decrease the CO2 in the blood…and vice-versa • For example, on conventional ventilation, a PIP of 24 and a PEEP of 4 results in a change in pressure of 20, and corresponds to a certain tidal volume…no different with high frequency ventilation
Circuit Positioning • The circuit should be tilted upward a few degrees to allow for water condensation to drain backward towards the ventilator. • The endotracheal tube should be kept as straight as possible to reduce any dampening of the pressure.
What do I do if the ventilator turns off? • The ventilator will automatically stop if there is a disconnect in the circuit, and may create profound, and perhaps life-threatening, alveolar collapse and oxygen desaturation. • Notify the RRT immediately. • Gently hand-bag the patient using appropriate inspiratory pressures (manometer), rate, and PEEP (PEEP valve) until the respiratory therapist arrives. • As with all patients receiving high frequency ventilation, any “elective” procedures such as suctioning, surfactant administration, and position changes require the presence of an RRT.
What’s that “chirping” noise? • “Chirping” or an intermittent alarm from the ventilator commonly occurs when the mean airway pressure has come close to the upper and lower alarm limits. • This is as a result of: • An improper alarm setting • Water spitting out of the control valve • Excessive respiratory effort from the patient • The MAP setting has been allowed to wander • Inadequate flow to meet the inspiratory demands of the patient.
Summary • High frequency ventilation can provide enhanced gas exchange beyond what is capable with conventional ventilation. • The open-lung or high-volume lung strategies have recently proven to be most successful with and without the presence of active air-leaks. • High frequency ventilation may provide a means of a lung “protective” strategy for ventilating patients with poor lung compliance at risk for developing air-leak syndromes. • High lung volume strategy coupled with the relatively stable intrathoracic volume may reduce venous return to the heart and decrease blood pressure. Some patients may benefit from an increase in intravascular volume and/or administration of medications that increase blood pressure. • Procedures such as suctioning, position changes, and surfactant administration are to be left for some time at which an RRT can be present, even if it means before or after the designated “stim” time.