Introduction to High Frequency Ventilation
Introduction to High Frequency Ventilation. Michael Haines, MPH, RRT-NPS, AE-C. Objectives. TYPES OF HFV There are four basic types of HFV: High frequency jet ventilation High frequency oscillatory ventilation High frequency percussive ventilation

Introduction to High Frequency Ventilation
E N D
Presentation Transcript
Introduction to High Frequency Ventilation Michael Haines, MPH, RRT-NPS, AE-C
Objectives • TYPES OF HFV • There are four basic types of HFV: • High frequency jet ventilation • High frequency oscillatory ventilation • High frequency percussive ventilation • High frequency positive pressure ventilation (RARE normal vent with high rates) • INO with HFV
Introduction • Respiratory insufficiency from ARDS remains a high risk for mortality. Intensification of conventional ventilation with higher rates and airway pressures leads to an increased incidence of barotrauma. Especially the high shearing forces resulting from large pressure amplitudes damage lung tissue. Either ECMO or high-frequency oscillatory ventilation might resolve such desperate situations. Since HFOV was first described by Lunkenheimer in the early seventies this method of ventilation has been further developed and is now applied the world over.
HFOV 3100 A – Neonates/Peds HFVO 3100 B- Adults
Introduction • HFV is a type of ventilation that delivers small tidal volumes (VT< VDS ) with supraphysiologic respiratory rates >150 bpm • The goal of HFV is to provide adequate ventilation/oxygenation in the presence of severe restrictive disease in order to prevent/reduce the risk of conventional ventilator induced lung injury • HFV uses momentum rather than airway • pressure to overcome lung compliance
Introduction • High-frequency ventilation was first introduced 30 years ago as a method for reducing intrathoracic pressure during thoracic and laryngeal surgery. High-frequency oscillation was developed in the 1970's for the treatment of lung disease of prematurity but is now used for acute hypoxemic respiratory failure in all ages.
Introduction • The key difference from CMV is the usage of high rates and low tidal volumes. Because the tidal volume is smaller than the dead space, the gas transport during HFV cannot be explained by bulk flow theory as in CMV. • HFV is not uncommon in nature and in fact occurs in: • Humming birds • Panting dogs
Introduction • Traditional wisdom: VA = f (VT - VDS) • Physiologic (effective) dead space can become < anatomic dead space »Animal studies of HFV: adequate ventilation can be achieved with VT as low as 1 ml/kg » Flow streaming reduces effective dead space - only portions of the anatomic DS are used » Fresh gas penetrates some alveoli
Introduction • During conventional ventilation direct alveolar ventilation accomplishes pulmonary gas exchange. According to the classic concept of pulmonary ventilation the amount of gas reaching the alveoli equals the applied tidal volume minus the deadspace volume. • At tidal volumes below the size of the anatomical deadspace this model fails to explain gas exchange. Instead, considerable mixing of fresh and exhaled gas in the airways and lungs is believed to be the key to the success of HFV in ventilating the lung at such very low tidal volumes.
Amplitude and Hertz • Amplitude (Power) height of wave • Hertz (frequency) how close each wave is
Hertz • Top: Hertz set at 3 • Bottom: 1 breath in conventional
Indications for Neonatal HFV • RDS non responsive to conventional ventilation • Prophylactic use is severe prematurity • PIE • PPHN • PN • Increase in intra-abdominal pressure e.g. NEC • MAS • CDH • TEF • HFV can be used as a prophylactic means of ventilation for extremely small neonates, but usually it is used after conventional ventilation has failed (Increased Paw, FIO2 demands, refractory hypoxemia, failure to ventilate, over distention, air leaks…). HFV may also be used in conjunction with NiO and ECMO therapy for patients failing to oxygenate.
Indications for HFV • Some criteria used are: PaCO2 >50 mmHg or FiO2 requirement greater than 0.5 to maintain PaO2 of 50 mmHg. • Oxygen index (OI =FiO2 * MAP /PaO2) >35 • PaO2/FiO2 ratio of less than 300 • Infants receiving HFV should be monitored continuously for their oxygenation and ventilation. They may require extra intravenous fluid to compensate the relative volume depletion resulting from redistribution of blood flow
Why we use HFV • It is safer and more effective to use smaller VT at higher PEEP (MAP) compared to larger VT at lower PEEP • HFV uses momentum rather than airway pressure to overcome lung compliance • Greatest benefit in diseases of poor lung • compliance • »Optimizing PEEP (MAP) during HFV is • critical
Why we use HFV • Indications • Rescue: This is the most established role for HFV • Prophylactic: In animal experiments HFV causes less lung injury than conventional ventilation. • Which do you think is better?
Normal (A and B) and acutely injured lung (C and D). Alveoli at peak inspiration (A) and end expiration (B) in the normal lung are very stable with little change in size during tidal ventilation (dots). High positive inspiratory pressure (PIP) and low PEEP injurious ventilation causes a ventilator-induced lung injury resulting in alveolar instability. Injured alveoli at peak inspiration (C) are inflated (dots) and totally collapse (arrows) end expiration (D), demonstrating severe instability during tidal ventilation.
In vivo photomicrographs of subpleural alveoli in the rat after lung injury by saline lavage ventilated with either conventional mechanical ventilation (CMV) or high-frequency oscillatory ventilation (HFOV) using a 2.5-internal diameter tracheal tube. With CMV, a group of alveoli are seen inflated during inspiration (dots) but collapse with expiration (arrows). Alveoli are very stable with HFOV during ventilation. The same alveolus is seen with HFOV at inflation and exhalation (dots).
Pulmonary Interstitial Lung Disease (PIE) Bulk flow to non compliant airways and alveoli increase distending pressure resulting in air leaks
Air leaks from the over stretching of non compliant alveoli can cause: • Subcutaneous emphysema • Pneumothorax • P.I.E. • Pneumomediastinum • Pneumo-pericardium • Pneumo-retroperitoneum • pneuomoperitoneum HFV is a method of mechanical ventilation that employs supra-physiological breathing rates and tidal volumes frequently less than dead space. Because conventional ventilation relies on the production of large pressure changes to induce mass flow of gas in and out of the lungs, it may be associated with deleterious consequences of volume and pressure changes at alveolar level. These include air leaks, such as PIE and pneumothorax, and bronchiolar-alveolar injury leading to chronic lung disease.
How does HFV work? • HFV enhances both bulk flow (convection) and diffusion of respiratory gases »Abundant fresh gas “washes out” expired gas from the airways »Decreased pCO2 at the gas exchange boundary increases diffusion • Linear relationship between ventilator rate • and CO2 elimination is no longer valid • »CV: CO2 = f x VT; HFV: CO2 = f x VT2 • »Changes in rate have less impact on gas • exchange than similar changes made during CMV Venegas and Fredberg: Crit Care Med 22 (suppl):S49, 1994
How does gas exchange occur with HFV • Direct ventilation of most proximal alveoli units by bulk convection • Direct Bulk Flow Some alveoli situated in the proximal tracheobronchial tree receive a direct flow of inspired air. This leads to gas exchange by traditional mechanisms of convective or bulk flow.
How does gas exchange occur with HFV • Pendalluft effect – asynchronous flow among alveoli due to asymmetries in airflow impedance. This causes gas to re-circulate among lung units and improve gas exchange. In healthy and, more so, in diseased lungs, the mechanics of air flow vary among lung regions and units within regions. Variation in regional airway resistance and compliance cause some regions to fill and empty more rapidly than others. Some gas may flow between regions if these characteristics vary among regions that are in close proximity. • Turbulence in the large airways causing enhanced gas mixing
How does gas exchange occur with HFV • Taylor dispersion – Turbulent eddies and secondary swirling motions occur when convective flow is superimposed on diffusion. Some fresh gas may mix with gas from alveoli, increasing the amount of gas exchange that would occur from simple bulk flow. • Collateral ventilation through non-airway connections between neighboring alveoli
How does gas exchange occur with HFV • Cardiogenic Mixing • Mechanical agitation from the contracting heart contributes to gas mixing, especially in peripheral lung units in close proximity to the heart. • Molecular Diffusion • As in other modes of ventilation, this mechanism may play an important role in mixing of air in the smallest bronchioles and alveoli, near the alveolocapillary membranes.
How does gas exchange occur with HFV • Asymmetric velocity – convective gas transport is enhanced by asymmetry between inspiratory and expiratory velocity profiles that occur at branch points in the airways. The velocity profile of air moving through an airway under laminar flow conditions is parabolic. Air closest to the tracheobronchial wall has a lower velocity than air in the center of the airway lumen. This parabolic velocity profile is usually more pronounced during the inspiratory phase of respiration because of differences in flow rates. With repeated respiratory cycles, gas in the center of the airway lumen advances further into the lung while gas on the margin (close to the airway wall) moves out toward the mouth
1. Direct bulk flow 2. Taylor dispersion 3. Pendeluft 4. Asymmetric velocity 5. Cardiogenic mixing 6. Molecular diffusion Chang, HK Mechanisms of gas transport during ventilation by high frequency oscillation. ;-563 Gas transport during HFV
Oxygenation with HFV • Oxygenation is determined by lung volume (affected by MAP) and FiO2. It is important to maintain adequate lung volume to prevent atelectasis and to preserve surfactant function to achieve adequate oxygenation. • Adequate MAP should be used to recruit alveoli and maintain lung volume above functional residual capacity (FRC). • In contrast to CMV, lung volume is maintained at a relatively constant level during HFV.
Oxygenation with HFV • The ventilation/perfusion matching would improve as a result of alveolar recruitment when lung volume increases. The near constant lung volumes in HFV results in better gas distribution and avoids the development of regional atelectasis in less compliant lung units, hence resulting in better ventilation/perfusion matching.
Adjustments of Ventilatory Settings During HFV • PaCO2 is reduced mainly by increase in HFV amplitude. • Changing the HFV frequency may have unpredictable effects on PaCO2 • Increasing the HFV frequency leads to a decrease in delivered tidal volume, and may result in an increase in PaCO2.
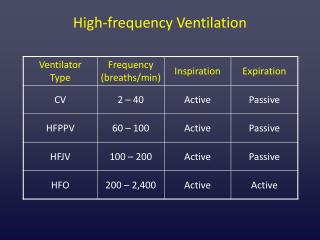
Types of HFV • Three types of HFV ventilators are approved for use in infants/adults in the United States, : • High frequency oscillatory ventilator (HFOV) • High frequency flow interrupter (HFFI) • High frequency jet ventilator (HFJV). • All forms of HFV have common characteristics: Respiratory rate >150 bpm Tidal volume= 1-3 mL/kg noncompliant ventilator circuits
HFOV • HFOV employs either a piston or diaphragm to oscillate a bias flow of gas to generate both positive and negative pressure fluctuations termed as amplitude. • The adjustable parameters include: • Power • IT% • Mean airway pressure (MAP) • Bias flow • Frequency (Hz) • Amplitude • Frequency is usually fixed for a particular patient group. • The recommended range is 10-15 Hz for premature infants and 8-10 Hz for term infants, around 5 Hz for adults
HFOV • Characterized by high respiratory rates between 3.5 to 15 hertz (210 - 900 breaths per minute), where 1 Hz=1 breath per second. • The rates used vary widely depending upon patient size, age, and disease process. Typically the smaller the patient the higher the Hz and vise versa. • Pressure oscillates around the constant distending pressure (equivalent to Mean Airway Pressure), which is usually set slightly higher than the MAP on conventional ventilation. • Gas is pushed into the lung during inspiration, and then pulled out during expiration (active exhalation).
HFOV • HFOV generates very low tidal volumes that are generally less than the dead space of the lung (watch for atelectasis and sudden drop in vital signs during implementation). • Tidal volume is dependent on endotracheal tube size, power and frequency.
HFOV • Different mechanisms of gas transfer are believed to come into play in HFOV compared to normal mechanical ventilation. • Often used in patients who have refractory hypoxemia that cannot be corrected by normal mechanical ventilation such as is the case in the following disease processes: severe ARDS, ALI and other oxygenation diffusion issues. In some neonatal patients HFOV may be used as the first-line ventilator due to the high susceptibility of the premature infant to lung injury from conventional ventilation.
HFOV Sensormedics 3100A http://www.youtube.com/watch?v=UgaDa4jNYP0&feature=related The 3100A has a diaphragmatically sealed piston driver. It is theoretically capable of ventilating patients up to 30 kg. Tidal volume typically delivered ≈ 1.5-3.0 ml/kg (< dead space). It is a efficient ventilator secondary to an active expiratory phase, but it is not capable of delivering sigh breaths for alveolar recruitment.
SensorMedics 3100A Oscillatory Ventilator • INITIAL SETTINGS: • FREQUENCY: Set initially at 10 Hz (600 BPM) for term infants and 15 Hz (900 BPM) for premature infants (< 2.5 kg). For children between 6-10 kg, use 8 Hz, and for children > 10 kg, use 6 Hz for an initial setting. • INSPIRATORY TIME (I.T.): Set initially at 33% (e.g. 22 milliseconds at 15 Hz, 41 milliseconds at 8 Hz, 55 milliseconds at 6 Hz). • 1) Warning - The percent of I.T. should seldom be increased because it will lead to air trapping and fulminate barotraumas. Total I.T. should only be increased by decreasing frequency, thus leaving the I:E ratio constant. I.T. can be decreased to 30% to heal air-leaks. • 2) I:E ratio: ≈ 1:2 for 3-15 Hz at 33% I.T. • The % Inspiratory time also controls the time for movement of the piston, and therefore can assist with CO2 elimination. • Increasing % Inspiratory Time will also affect lung recruitment by increasing delivered Paw.
SensorMedics 3100A Oscillatory Ventilator • POWER (AMP): A rough representation of the volume of gas generated by each high frequency wave. Range (1.0 - 10.0). • Maximum amplitude or volume delivered is highly variable and depends on: circuit tubing (compliance, length and diameter), humidifier (resistance and compliance - water level), ET tube diameter and length • 1) Set the POWER initially at 2.5 if wt <2.0 kg, 3.0 if wt < 2.5 kg, 4.0 if wt 2.5 - 4.0 kg, 5.0 if wt 4.0 - 5.0 kg, 6.0 if wt < 10 kg, 7.0 if wt > 20 kg. • Check ABG's every 15-20 min until PaCO2≈ 40-60, i.e., titrate POWER setting based on PaCO2 desired. • Chest wall needs to be vibrating. If not vibrating, increase power. • 2) Alveolar ventilationis directly proportional to POWER, so the level of PaCO2 is inversely proportional to the power.
SensorMedics 3100A Oscillatory Ventilator • Amplitude is a measurement created by the force that the piston moves which is based on the POWER setting, resulting in a volume displacement and a visual CHEST WIGGLE. It is represented by a peak to- trough pressure swing across • the mean airway pressure.
SensorMedics 3100A Oscillatory Ventilator • MAP: Initial MAP 4 cm above MAP while on CMV • Oxygenation on HFOV is directly proportional to MAP, which is similar to CMV, however with the SensorMedics HFOV the MAP is generated by PEEP. Thus during HFOV: MAP = PEEP. • 1. Initial MAP Settings: • a) Neonates - Initial MAP should be 2-4 cm above the MAP on CMV. • b) Infants/Children - Initial MAP should be 4-8 cm above the MAP on CMV. • c) If starting immediately on HFOV - use a MAP of ≈ 8-10 cm in neonates and 15-18 cm in infants/children. • Check CXR 2 hrs after converting to HFOV, then adjust MAP to achieve optimal lung volume (9-10 ribs expanded). • If not oxygenating, increase MAP by 2 cm every hour until oxygenation improves. Adjust Power to keep PaCO2 45-55.
Sensormedics 3100B ://www.youtube.com/watch?v=jLroOPoPlig
SensorMedics 3100B Oscillatory Ventilator • Initial Settings and Suggestions for Larger Patient Use On 3100 B • Patients with ARDS >35 Kg • Set Paw 5 cmH20 above CV Paw • FiO2 100% • Set Hertz at 5-6 • Power 4.0, adjust for good chest wiggle • I time % at 33% • Set Bias Flow at >25 lpm, may need to go higher
SensorMedics 3100B Oscillatory Ventilator • Guidelines for Initial HFOV Settings: • 1. Prior to initiating HFOV, perform a recruitment maneuver on the oscillator by increasing Paw to 40 cmH2O for 30-40 seconds. NOTE: the oscillator should be OFF during the maneuver. Immediately abort the maneuver if hemodynamic compromise occurs. • 2. Set initial Paw at 5 cmH2O above conventional ventilator Pmaw. • 3. Set power to achieve initial amplitude at chest oscillation to mid-thigh. • 4. Set Hz at 5. Set IT to 33% (may increase to 50% if difficulty with oxygenation; this may further raise carinal pressure an additional 2 – 4 cmH2O). • 5. If oxygenation worsens, increase Pmaw in 2 – 3 cmH2O increments q 30 minutes until maximum setting (approximately 45 – 55 cmH2O).