Download
1 / 60
740 likes | 1.38k Vues
INTRAOPERATIVE RADIATION THERAPY (IORT) for EARLY-STAGE BREAST CANCER Dr. Maria C.E. Jacobs Director, Radiation Oncology Mercy Medical Center Baltimore, Maryland. EARLY-STAGE BREAST: Local Breast Treatment. BCT consisting of conservative surgery (CS) with lumpectomy/partial mastectomy and RT

E N D
INTRAOPERATIVE RADIATION THERAPY (IORT)for EARLY-STAGE BREAST CANCERDr. Maria C.E. JacobsDirector, Radiation OncologyMercy Medical CenterBaltimore, Maryland
EARLY-STAGE BREAST: Local Breast Treatment • BCT consisting of conservative surgery (CS) with lumpectomy/partial mastectomy and RT • Mastectomy +/- immediate reconstruction
BREAST CONSERVATION THERAPY:Treatment Objectives • Optimize local control • Minimize acute and long-term complications • Maintain optimal cosmesis
Breast Conservation Therapy (BCT) is a standard of care supported by years of data. • BCT refers to breast-conserving surgery (BCS) + radiotherapy. • 27+ years of data support BCT as a standard of care. • Six modern, prospective randomized trials found no significant differences when comparing BCT to mastectomy. • Clinical trials compared local recurrence, distant metastasis, and long-term survival.
NCI (Milan) NSABP B-06 NCI (France) NCI (USA) EORTC Danish Group RANDOMIZED TRIALS COMPARING MASTECTOMY vs. BCT
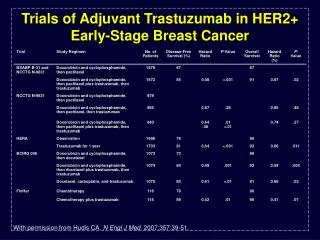
Prospective Randomized Trials comparing Mastectomy (M) vs. BCT Trial No. of Pts %Local Recurrence %Survival F/U Interval BCT M BCT M (YR) NASBP 1219 12 8 63 59 15 MILAN 701 7 4 65 65 18 NCI 237 16 6 77 75 10 EORTC 868 20 12 65 66 10 IGR 179 9 14 73 65 15 DBCG 904 5 6 79 82 6
Summary of Randomized Trials:BCT vs. Mastectomy • Continuous follow-up demonstrates NO significant differences between BCT and mastectomy in: - loco-regional control - distant metastases - overall survival • No disadvantage in the use of BCT for patients with positive axillary lymph nodes • No significant differences in the rate of second malignancies or contralateral breast cancer
Critical Elements in the Selection of Patients for BCT • History and Physical Exam: - Age should not be a contraindication for BCT - Comorbid conditions should be considered prior to BCT - Locally-advanced disease • Radiological Evaluation: - Multicentricity - Extent of calcifications
Critical Elements in the Selection of Patients for BCT • Pathologic Evaluation: - Positive axillary lymph nodes are NOT a contraindication for BCT - NEGATIVE margins of resection • Needs and Expectations: - Self-esteem/Sexuality - Sense of disease control - Functionality - Overall quality of life
Contraindications for BCT • Absolute: - More than two primaries in separate quadrants - Diffuse and pleomorphiccalcifications - History of previous RT to the breast - Pregnancy in the first and second trimesters. Surgery can be performed in third trimester and RT can be deferred until after delivery - Persistent positive margins of resection after “reasonable” surgical attempts
Contraindications for BCT • Relative: - History of collagen vascular disease. Scleroderma and active systemic lupus are ABSOLUTE contraindications - Large tumor in small breast - Large and pendulous breast preventing daily reproducibility and dose homogeneity
Non-Mitigating Factors in the Selection of Patients for BCT (factors not affecting acceptability) • Family history of breast cancer is NOT a contraindication for BCT • BRCA 1 and 2 mutations are NOT a contraindication for BCT • High risk for systemic relapse is NOT a contraindication for BCT. It is a determinant for adjuvant systemic management • BCT can be offered to patients with positive axillarylymph nodes
Radiation Therapy for Early-Stage Breast Cancer (post-lumpectomy) • Whole Breast Irradiation for 4500-5000 centiGrayin 25-28 daily fractions of 180-200 centiGray/fraction • Tangential fields, 6-18 MV photon beam • “Boost” for 1500-2000 centiGray in 8-10 fractions using an electron beam or “mini-tangential fields depending on tumor bed depth
Standard Breast Irradiation:Side Effects and Long-Term Complications • Acute - Skin: discoloration, dry and moist desquamation - Fatigue - Anemia is rare • Long-Term - Arm and breast edema - Myositis - Pneumonitis
Under-Utilization of BCT 240,000 Breast Cancer Cases in 20071 ~180,000 Eligible for Breast Conservation Therapy (BCT)2 a ~72,153 40% ~73,957 41% Mastectomy BCT Lumpectomy No Radiation 108,2303 ~34,273 19% No Radiation Eligible for lumpectomybut receive mastectomy Receive BCT Lumpectomy + WBRT or APBI Source: 12007 Cancer Facts & FiguresAmerican Cancer Society 2U.S. Department of Health and Human Services, Office on Women’s Health 3SEER Data 2000-2004 Incidence Rates, NCI Receive BCS w/o Radiation
Women Eligible for Breast Conservation Therapy 19% lumpectomy w/o radiation.1 Reasons cited:3 - Limited radiotherapy resources - Treatment-related morbidity - Loss of income due to prolonged treatment duration with radiation • 41% mastectomies1 • Reasons cited:2 • - Time commitment • - Inconvenience • - Fear of radiation • - Treating physician bias • 46% with DCIS have lumpectomy alone.4 • Causative factors associated with under-treatment include issues with transportation, insurance coverage, employment and physicallimitations.5 1Cancer Trends Progress Report - 2005 Update, National Cancer Institute, NIH, DHHS, Bethesda, MD, December 2005, http://progressreport.cancer.gov. 2Keisch ME. Breast Cancer Res. 2005;7:106-109. 3Vinh-Hung et al. J Nat Cancer Inst. 2004:96:115-121. 4Baxter et al. J Natl Cancer Inst. 2004;96:443-448. 5Jeruss et al. Ann SurgOncol. 2006;13:967-976.
Several randomized trials have been conducted to determine if radiation therapy (RT) can be omitted after breast-conserving surgery. No subset of patients has been identified that can conclusively be treated with surgery alone. Is it Safe to Omit Radiation Therapy After BCS? 1 Baxter et al. J Natl Cancer Inst. 2004;96:443-448. 2 Burstein et al. N Engl J Med. 2004;350:1430-1441. 3 Houghton et al. Lancet. 2003;362:95-102. 4 Julien et al. Lancet. 2000;355:528-533. 5 Fisher et al. N Engl J Med. 1993;328:1581-1586.
Is Excision Alone Adequate in Any Subset of Patients • According to previous clinical trials, all subsets of patients benefit from RT • Risk factors for local recurrence after lumpectomy alone include tumor size, margins, grade, EIC and receptor status • A very selected group of patients may not require RT • RT is still STANDARD following CS
CS vs. CS AND RT for Early-Stage Breast Cancer: Impact of RT Trial % Local Recurrence %Reduction (Recurrence) CS CS+RT CS vs. CS+RT NSABP 36 12 67 Ontario 35 11 69 Milan 24 6 75 Scottish 25 6 76 English 35 13 63 Uppsala-Orebro 24 9 63
Prospective Trials comparing CS vs. CS and RT • These trials have variables including extent of the surgical resection (wide excision vs. quadrantectomy) and length of follow-up • However, they all show a substantial reduction in the local recurrence rate with the addition of radiotherapy
Is Excision Alone Adequate in Any Subset of Patients • According to previous clinical trials, all subsets of patients benefit from RT • Risk factors for local recurrence after lumpectomy alone include tumor size, margins, grade, EIC and receptor status • A very selected group of patients may not require RT • RT is still STANDARD following CS
New/Alternative Treatment Approaches • Is excision alone adequate therapy? • Is the “boost” necessary? • Is partial breast irradiation an acceptable treatment modality? • Is accelerated partial breast irradiation (APBI) an acceptable option?
How Did the Concept of Accelerated Partial Breast Irradiation Originate? • Findings suggest that the major benefit of radiation therapy is derived from radiation directed at the breast tissue immediately surrounding the lumpectomy site.1 • The majority of local recurrences after breast-conserving therapy occur at or near the tumor bed.1 • The incidence of “elsewhere” failures appears to be unaffected by whole breast irradiation: 1-5% of patients fail elsewhere regardless of radiation.1,2 • Whole breast irradiation may not be needed in appropriately selected patients.2 1King et al. Am J Surg. 2000;180:299-304. 2Arthur et al. Brachytherapy. 2002;1:184-190.
“Elsewhere” Failures • Incidence of failures outside of tumor bed in randomized trials comparing lumpectomy with or without postoperative irradiation.1 The data suggest WBRT does not protect against new disease development elsewhere in the breast. 1Baglan et al. Int J RadiatOncolBiol Phys. 2001;50:1003-1011.
Imamura Ohtake 40-64 >64 ≥50 100% ISO 100% ISO 75% ISO 75% ISO Disease Extension Illustrated Imamura1: Max 8.32 mm Ohtake2: Max 7.7 mm Red Line is MammoSite Radiation Prescription Depth at 100% Isodose: 1 cm. Green line is 75% Isodose. 1Imamura et al. Breast Cancer Res Treat. 2000;62:177-184. 2Ohtake et al. Cancer. 1995;76:32-45.
Accelerated Fractionation Schedules:Partial Breast Irradiation • Brachytherapy • External Beam Radiotherapy • Intraoperative Radiotherapy
APBI Techniques External Beam for APBI CONTURA MammoSite Interstitial multi-catheter SAVI
Breast Brachytherapy Scientific Rationale • Published data reports low local recurrence rates, ranging from • 0.0 - 4.4 %, • in patients treated with brachytherapy as primary treatment.
Interstitial Brachytherapy –Multi-Entry/Multi-Catheter Arthur and Vicini, 2005
Published Data on Breast Brachytherapy as Primary Treatment: > 5-year Median Follow-up 1 King et al. Am J Surg. 2000;180: 299-304.2Vicini et al. JNCI. 2003;95:1205-1210.3Polgar et al. Int J RadiatOncolBiol Phys. 2007;69:694-702.
William Beaumont Hospital Trial: Cosmetic Outcomes with APBI1 • Population: 199 consecutive patients with invasive early-stage (I–II) breast carcinoma. • Treatment: Hypofractionated APBI using interstitial brachytherapydirected only at the region of the tumorbed. 1Chen et al. Cancer. 2006;106(5):991-999.
MammoSite Rationale • 2002 IJROBP MammoSite • Dosimetry Publication: • Presents dosimetric characteristics of MammoSite • Analysis by William Beaumont, leader in breast brachytherapy • Key findings comparing MammoSite to multicatheter interstitial brachytherapy: • - Favorable volume coverage and reproducibility
MammoSite –Single Entry/Single Catheter Arthur and Vicini, 2005
Contura Applicator- Single Entry/Multi-Catheter PTVforContura Balloon MammoSite
SAVI Applicator – Single Entry/Multi-Catheter
ABS and ASBS Patient Selection Criteria ≥ 50 ≥ 45 Invasive ductal carcinoma or DCIS Infiltrating ductal carcinoma ≤ 3 cm ≤ 3 cm Negative microscopic surgical margins of excision Negative microscopic surgical margins of excision NØ NØ 1American Brachytherapy Society, Breast Brachytherapy Task Group, February 2007. 2Consensus statement for accelerated partial breast irradiation. American Society of Breast Surgeons, 2005.
NSABP B-39 /RTOG 0413: Phase III Trial *NSABP B-39 enrollment now closed to lower risk patients: DCIS patients ≥ 50 years AND Invasive Breast Cancer patients ≥ 50 years who are node negative and hormone-receptor positive.
ACCELERATED PARTIAL BREAST IRRATDIATON • Reduction of treatment time from 6-7 weeks to 5 days • It decreases the target volume (lumpectomy plus 1-2 cm margin • Increases dose per fraction: 340 cGy twice daily (BID) x 5 days= 3,400 cGy • Use highly conformal dose delivery using CT based 3D-CRT
Lessons learned from APBI Patient Appeal Decreased Overall Treatment Time: Radiotherapy: 1 week vs. 6-7 weeks CS--chemotherapy (4-6 months)--RT(6-7weeks) VS. CS------- RT (1 week) ------- Chemotherapy Less skin toxicity Less systemic toxicity
INTRAOPERATIVE RADIATION THERAPY(IORT): DEFINITION Intraoperative Radiation Therapy (IORT) is the delivery of a single high dose of radiation to the target area/tumor bed at the time of surgery.
IORT It is TRULY a multidisciplinary approach during which the surgeon removes the tumor and the radiation oncologist directs the radiation to the tumor bed, with both physicians working together, hand in hand, to spare surrounding normal tissues.
IORT IORT is NOT a new approach to cancer management. As the result of pioneering work by Dr. Abe in Kyoto, Japan, IORT using linear accelerators has been used in the U.S.A., Europe and Japan for the treatment of malignancies in the abdomen (sarcomas, rectum, gynecologic and retroperitoneal tumors)
IORT: History • 1909: Beck treated a patient with colon cancer using low-energy X-rays • Early 1970, Dr. Abe in University of Kyoto, Japan • 1978, IORT pioneered in the U.S.A.: - Howard University/N.C.I., Washington, D.C. - Massachusetts General Hospital
Why IORT? • Partial breast Irradiation experience promising excellent local control and acceptability by patients • Single fraction • Treatment delivered in sterile environment, reducing risk for infection • AIMING RADIATION where RADIATION IS NEEDED
Intraoperative Radiation Devices Ash, RB, et al, Oncology, 107 (2013)
IORT Systems of kV versus MV Devices Carl Zeiss INTRABEAM and XoftAxxenteBxvsIntraOp Medical Mobetron
Arm stand with x-ray source X-ray source Control Workstation Carl Zeiss IORT IntraBeam System
Applicator on the x-ray source Solid applicator and balloon Solid applicator size available: 1.5, 2.0, 2.5, 3.0, 3.5, 4.0, 4.5, 5.0 cm in diameter, labeled by A, B, C, D, E, F, G, and H for the part number. Reusable 100 times. Balloon size available: 3.0, 3.5, 4.0, 4.5, 5.0 cm in diameter. Single use.
Spatial distribution of X-ray beam 50 kV, 40 µA -1.5 mm 0 +1.5 mm 7 6 5 4 3 2 1 Gy/min
Step 1: The lumpectomy, immediately following tumor removal. Step 2: After the surgeon has removed the tumor, the radiation oncologist positions the INTRABEAM applicator in the area of the breast where the tumor was located. Step 3: Low energy radiation is delivered locally to the targeted tissue in the tumor bed, minimizing healthy tissue exposure to radiation. Step 4: After 20-30 minutes of radiotherapy, the applicator is removed and the surgeon then closes the incision. IORT Procedure with Solid Applicator