WORLD HEALTH ORGANIZATION
WORLD HEALTH ORGANIZATION. WHO FUNCTION.


WORLD HEALTH ORGANIZATION
E N D
Presentation Transcript
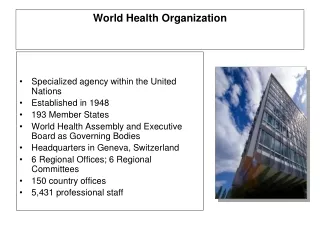
WHO FUNCTION • WHO is the directing and coordinating authority for health within the United Nations system. It is responsible for providing leadership on global health matters, shaping the health research agenda, setting norms and standards, articulating evidence-based policy options, providing technical support to countries and monitoring and assessing health trends. • In the 21st century, health is a shared responsibility, involving equitable access to essential care and collective defence against transnational threats.
GOVERNANCE/WORLD HEALTH ASSEMBLY • The World Health Assembly is the supreme decision-making body for WHO. It generally meets in Geneva in May each year, and is attended by delegations from all 193 Member States. Its main function is to determine the policies of the Organization. The Health Assembly appoints the Director-General, supervises the financial policies of the Organization, and reviews and approves the Proposed programme budget. It similarly considers reports of the Executive Board, which it instructs in regard to matters upon which further action, study, investigation or report may be required.
THE EXECUTIVE BOARD • The Executive Board is composed of 34 members technically qualified in the field of health. Members are elected for three-year terms. The main functions of the Board are to give effect to the decisions and policies of the Health Assembly, to advise it and generally to facilitate its work. • The Secretariat of WHO is staffed by some 8000 health and other experts and support staff on fixed-term appointments, working at headquarters, in the six regional offices, and in countries. • The Organization is headed by the Director-General, who is appointed by the Health Assembly on the nomination of the Executive Board.
WHO AGENDA • “I WANT MY LEADERSHIP TO BE JUDGED BY THE IMPACT OF OUR WORK ON TWO POPULATIONS : WOMEN AND THE PEOPLE OF AFRICA” …DR MARGARET CHAN, DIRECTOR GENERAL.
WHO: PROMOTING DEVELOPMENT • During the past decade, health has achieved unprecedented prominence as a key driver of socioeconomic progress, and more resources than ever are being invested in health. Yet poverty continues to contribute to poor health, and poor health anchors large populations in poverty. Health development is directed by the ethical principle of equity: Access to life-saving or health-promoting interventions should not be denied for unfair reasons, including those with economic or social root. • WHO activities aimed at health development give priority to health outcomes in poor, disadvantaged or vulnerable groups. • CORNERSTONES OF THE HEALTH AND DEVELOPMENT AGENDA • Attainment of the health-related Millennium Development Goals, • Preventing and treating chronic diseases and • Addressing the neglected tropical diseases.
WHO: FOSTERING HEALTH SECURITY • 2. Fostering health security • Shared vulnerability to health security threats demands collective action. One of the greatest threats to international health security arises from outbreaks of emerging and epidemic-prone diseases. Such outbreaks are occurring in increasing numbers, fuelled by such factors as rapid urbanization, environmental mismanagement, the way food is produced and traded, and the way antibiotics are used and misused. The world's ability to defend itself collectively against outbreaks has been strengthened since June 2007, when the revised International Health Regulations came into force.
WHO: STRENGTHENING HEALTH SYSTEMS • 3. Strengthening health systems • For health improvement to operate as a poverty-reduction strategy, health services must reach poor and underserved populations. Health systems in many parts of the world are unable to do so, making the strengthening of health systems a high priority for WHO. Areas being addressed include the provision of adequate numbers of appropriately trained staff, sufficient financing, suitable systems for collecting vital statistics, and access to appropriate technology including essential drugs.
WHO: HARNESSING RESEARCH… • 4. Harnessing research, information and evidence • Evidence provides the foundation for setting priorities, defining strategies, and measuring results. WHO generates authoritative health information, in consultation with leading experts, to set norms and standards, articulate evidence-based policy options and monitor the evolving global heath situation.
WHO: ENHANCING PARTNERSHIP • 5. Enhancing partnerships • WHO carries out its work with the support and collaboration of many partners, including UN agencies and other international organizations, donors, civil society and the private sector. WHO uses the strategic power of evidence to encourage partners implementing programmes within countries to align their activities with best technical guidelines and practices, as well as with the priorities established by countries.
WHO: IMPROVING PERFORMANCE • 6. Improving performance • WHO participates in ongoing reforms aimed at improving its efficiency and effectiveness, both at the international level and within countries. WHO aims to ensure that its strongest asset - its staff - works in an environment that is motivating and rewarding. WHO plans its budget and activities through results-based management, with clear expected results to measure performance at country, regional and international levels.
WHO: GLOBAL BURDEN OF DISEASE Global Burden of Disease (GBD) 2010 study WHO is participating in a multi-center collaboration to revise and update global estimates of burden of disease, injury and risk factors for the years 1990 and 2005. Many WHO staff members are involved this project: participating in core planning of the project; providing access to WHO databases and providing expertise on specific diseases, injuries, and risk factors. • The Bill & Melinda Gates Foundation has provided funding for a new round of the Global Burden of Disease study, the GBD 2010 study, to be published in 2011. The study is led by the Institute for Health Metrics and Evaluation (IHME) at the University of Washington, with key collaborating institutions including WHO, Harvard University, Johns Hopkins University and the University of Queensland. The GBD 2010 study will develop improved methods to make full use of the increasing amount of health data, particularly from developing countries, and will include a comprehensive and consistent revision of disability weights. The study will also assess trends in the Global Burden of Disease from 1990 to 2005.
WHO: ESSENTIAL DRUGS • The essential medicines list is an inventory of medicines that treat pressing global health concerns. Medicines are identified through an evidence-based process and quality, safety, efficacy and cost-effectiveness are key selection criteria. A model list - first assembled by a World Health Organization (WHO) expert panel in 1977 and revised every two years to reflect current health challenges - gives Member Countries an example to adapt to national needs. • In 1977 the first list identified 208 essential medicines to battle the global disease burden at the time. Today's list of 340 medicines treats such priority conditions as malaria, HIV/AIDS, tuberculosis, reproductive health and, increasingly, chronic diseases such as cancer and diabetes.
WHO ON ALCOHOL • Although alcohol consumption has occurred for thousands of years, many of the varied health effects have been discovered fairly recently. Alcohol consumption has health and social consequences via intoxication (drunkenness), dependence (habitual, compulsive and long-term drinking), and other biochemical effects. In addition to chronic diseases that may affect drinkers after many years of heavy use, alcohol contributes to traumatic outcomes that kill or disable at a relatively young age, resulting in the loss of many years of life to death or disability. There is increasing evidence that besides volume of alcohol, the pattern of the drinking is relevant for the health outcomes. Overall there is a causal relationship between alcohol consumption and more than 60 types of disease and injury. Alcohol is estimated to cause about 20-30% worldwide of oesophageal cancer, liver cancer, cirrhosis of the liver, homicide, epilepsy, and motor vehicle accidents.
WHO ON ALCOHOL • Globally alcohol consumption has increased in recent decades, with all or most of that increase in developing countries. This increase is often occurring in countries with little tradition of alcohol use on population level and few methods of prevention, control or treatment. The rise in alcohol consumption in developing countries provides ample cause for concern over the possible advent of a matching rise in alcohol-related problems in those regions of the world most at risk. • Worldwide alcohol causes 2.5 million deaths (3.8 % of total) and 69.4 million (4.5 % of total) of Disability-Adjusted Life Years (DALYs). Unintentional injuries alone account for about one third of the 2.5 million deaths, while neuro-psychiatric conditions account for close to 40% of the 69.4 million DALYs. The burden is not equally distributed among the countries.
WHO:HEALTH RISK OF MOBILE PHONES Given the immense number of people who use mobile phones, even a small increase in the incidence of adverse effects on health could have major public health implications. • Because exposure to the radiofrequency (RF) fields emitted by mobile phones is generally more than a 1000 times higher than from base stations, and the greater likelihood of any adverse effect being due to handsets, research has almost exclusively been conducted on possible effects of mobile phone exposure. • Research has concentrated on the following areas: • cancer • traffic accidents • electromagnetic interference • other health effects. • Conclusions: No recent national or international reviews have concluded that exposure to the RF fields from mobile phones or their base stations causes any adverse health consequence. However, areas have been identified by the WHO's EMF Project for further research to better assess health risks and have led to over US$ 250 million in research worldwide to study RF effects on health. It will take about 2-3 years for the required RF research to be completed, evaluated and to publish an updated WHO health risk assessment.
WHO ON CLONING • 1. What is a clone? • The term clone, from the Greek for “twig,” denotes a group of identical entities; in recent years, “clone” has come to mean a member of such a group and, in particular, an organism that is a genetic copy of an existing organism. The term is applied by scientists not only to entire organisms but to molecules (such as DNA) and cells.
WHO ON CLONING • Why did scientists develop cloning techniques? • Scientists were initially interested in SCNT as a means of determining whether all the genes in an organism’s genome remain functional even after most of them have been switched off as a developing organism’s cells assume their specialized functions as blood, bone, muscle, and so forth. The ability of scientists to stimulate the DNA in a nucleus from a fully differentiated cell to revert to a condition comparable to the DNA in a newly fertilized egg and to begin the process of embryonic development demonstrated that all the genes remain viable in differentiated cells even though only a few genes are actually expressed in each cell. Commercial interest in animal cloning centres on replicating large numbers of genetically identical animals, especially those derived from a progenitor which has been modified genetically. In this fashion, mice or other laboratory animals that exhibit particular conditions can be created for specialized studies, or herds of farm animals (such as goats, sheep, or cows) can be created all of whom produce pharmaceutically useful proteins in their milk.
WHO ON CLONING • How does “Dolly type” cloning occur? • To produce Dolly, the researchers used an improved version of the technique of somatic-cell nuclear transfer (SCNT) first used 40 years ago in research with tadpoles and frogs. SCNT begins with an adult somatic cell, for example, a skin cell. “Adult” means a fully differentiated cell from an organism that had passed the embryonic stage of development, and “somatic” denotes a body cell (rather than an egg or sperm cell), which possesses the full complement of chromosomes, rather than the half contained in gametes. The nucleus from the somatic cell is transferred to an enucleated egg (that is, one from which the nucleus has been removed). The egg is then activated with electric current or chemicals in order to stimulate it to divide. When the blastocyst stage has been reached, the embryo is transferred into the uterus of a female host, where – if implantation occurs – it can lead to a pregnancy and eventually to the birth of an individual that carries the same nuclear genetic material as the donor of the adult somatic cell. Animals created through SCNT are not precise genetic copies of the donors of their nuclear DNA, however, since a small amount of DNA resides in the mitochondria outside the egg's nucleus; mitochondrial DNA is normally passed on to children only from their mothers. Since a clone would derive its mitochondrial DNA from the egg, not from the donor of the nucleus, the clone and its progenitor would be genetically identical only if the egg came from the progenitor or from the same maternal line.
WHO ON CLONING What is WHO’s position on cloning to replicate a human being (“human reproductive cloning”)? • The Member States of the World Health Organization (WHO) consider that developments in human reproductive cloning have unprecedented ethical implications and raise serious concerns for the safety of individuals and subsequent generations of human beings. The World Health Assembly has therefore resolved that the use of cloning "for the replication of human individuals is ethically unacceptable and contrary to human dignity and integrity."
WHO ON CLONING What justifications are offered for non-reproductive human cloning? • Scientists engaged in cloning for research argue that it presents a unique method for studying genetic changes in cells derived from patients suffering from such diseases as Parkinson’s disease, Alzheimer’s disease, and diabetes. Scientists who are interested in such research look ahead to the day when they believe that embryonic stem cells will be used to assist drug development and evaluation, for diagnostic purposes, and to create cells and tissues for transplantation. For the latter, if the stem cells used in transplantation were derived from embryos cloned from the patient needing the transplant, they might be less subject to rejection than cells, tissues or organs from another person, since the DNA in the cloned cells would be nearly identical to the patient’s own.