Download
1 / 65
660 likes | 866 Vues
Low-Dose Aspirin for the Primary Prevention of Atherosclerotic Events in Patients With Type 2 Diabetes A Randomized Controlled Trial. Hisao Ogawa, MD, PhD Department of Cardiovascular Medicine Graduate School of Medical Sciences Kumamoto University Kumamoto, Japan.

E N D
Low-Dose Aspirin for the Primary Prevention of Atherosclerotic Events in Patients With Type 2 Diabetes A Randomized Controlled Trial Hisao Ogawa, MD, PhD Department of Cardiovascular Medicine Graduate School of Medical Sciences Kumamoto University Kumamoto, Japan นส.ภ.ศิรินภา โคตรจันทร์ นส.ภ.อมรรัตน์ เต็มวงษ์ นศภ.วิชากร เกื้อก่อยอด Ambulatory care
Outline • ที่มาและความสำคัญ • ขั้นตอนการเลือกงานวิจัย • Abstract • Background • Method • Results • Comment
ที่มาและความสำคัญ • ปัจจุบันมีการใช้ Aspirin เพื่อป้องกัน Atherosclerotic ในผู้ป่วยเบาหวานชนิดที่ 2 จำนวนมาก • การใช้ Aspirin ขนาดต่ำสามารถป้องกันการเกิด Atherosclerotic ในผู้ป่วยเบาหวานได้หรือไม่?
ขั้นตอนการเลือกงานวิจัยขั้นตอนการเลือกงานวิจัย MeSH: Aspirin, Diabetes mellitus, Atherosclerotic Total paper 6 trial Limit : English
Impact factor = 31.7 JAMA, November 12, 2008—Vol 300, No. 18
Author Hisao Ogawa, MD, PhD Department of Cardiovascular Medicine Graduate School of Medical Sciences,Kumamoto University, Kumamoto, Japan Coauthors Masafumi Nakayama, Takeshi Morimoto, ShiroUemura, Masao Kanauchi, NaofumiDoi, Hideaki Jinnouchi, Seigo Sugiyama, Yoshihiko Saito
Financial Disclosures • Grant support for JPAD from Ministry of Health, Labour and Welfare (Japan) • Grant support from Astellas, AstraZeneca, Banyu, Bayer Yakuhin, Boehringerlngelheim, Cathex, Chugai, Daiichi Sankyo, Dainippon Sumitomo, Eisai, Get Bros., Guidant Japan, Japan Lifeline, Kaken, Kissei, Kowa, Kyowa Hakko, Mitsubishi Tanabe, Mochida, Nihon Kohden, Nihon Schering, Novartis, Otsuka, Pfizer, Pharmacia, Sankyo, Sanofi-Aventis, Sanwa Kagaku Kenkyusho, Schering-Plough, Sionogi, Sumitomo, Taisho Toyama, Takeda, Mitsubishi Tanabe, Teijin, Toa Eiyo, Torii, Toyama, Tyco Healthcare Japan, Vitatron Japan, Zeria, Novo Nordisk, Higo Foundation for Promotion of Medical Education and Research, Japan Foundation of Applied Enzymology, Japan Heart Foundation, Japanese Society of Interventional Cardiology, Kimura Memorial Heart Foundation, Kumamoto Medical Society, Smoking Research Foundation and Takeda Science Foundation for the past 5 years. No other potential conflict of interest relevant to this study was reported.
1 ชื่อเสียงของวารสารที่ตีพิมพ์บทความดังกล่าวเป็นอย่างไร มีคณะกรรมการที่มีความรู้ ความสามารถเหมาะสมทำการประเมินทางวิชาการหรือไม่ • มีความเหมาะสม เนื่องจากบทความตีพิมพ์ในวารสาร Journal of American Medical Association (JAMA) ซึ่งเป็นวารสารที่มีชื่อเสียงและเป็นที่ยอมรับแพร่หลาย
2 ชื่อของบทความ มีการสื่อความหมายไปในทำนองเดียวกันกับบทความหรือไม่ ผู้เขียนมีการแสดงอคติหรือไม่ Low-Dose Aspirin for the Primary Prevention of Atherosclerotic Events in Patients With Type 2 Diabetes A Randomized Controlled Trial • ชื่อบทความมีความเอนเอียง อาจทำให้ผู้อ่านเข้าใจว่า การใช้ low-dose aspirin สามารถป้องกันการเกิด Atherosclerosis ได้
3 คุณสมบัติของผู้ทำการวิจัย เหมาะสมที่จะดำเนินการศึกษาเชิงทดลองทางคลินิกเรื่องดังกล่าวหรือไม่ Hisao Ogawa, MD, PhD Department of Cardiovascular Medicine Graduate School of Medical Sciences,Kumamoto University, Kumamoto, Japan ผู้แต่งมีความเชี่ยวชาญด้าน Cardiovascular
4 ผู้สนับสนุนค่าใช้จ่ายในการศึกษาคือหน่วยงานใด มีส่วนที่ทำให้เกิดอคติต่อผลการศึกษาหรือไม่ Financial Disclosures: • Grant support for JPAD from Ministry of Health, Labour and Welfare (Japan) • Grant support from Astellas, AstraZeneca, Banyu, Bayer Yakuhin, Boehringerlngelheim, Cathex, Chugai, Daiichi Sankyo, Dainippon Sumitomo, Eisai, Get Bros., Guidant Japan, Japan Lifeline, Kaken, Kissei, Kowa, Kyowa Hakko, Mitsubishi Tanabe, Mochida, Nihon Kohden, Nihon Schering, Novartis, Otsuka, Pfizer, Pharmacia, Sankyo, Sanofi-Aventis etc. ไม่น่าจะก่อให้เกิดอคติต่อผลการศึกษา เนื่องจากมีหน่วยงานที่สนับสนุนทั้งภาครัฐและเอกชน อีกทั้งยา Aspirin ไม่ใช่ยาใหม่ที่จะเกิดผลประโยชน์แก่บริษัทผู้ผลิต
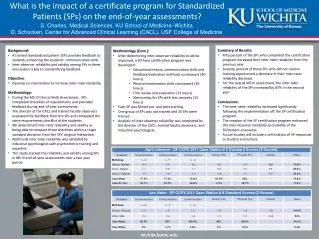
7 บทคัดย่อครอบคลุมหัวข้อ Objective, Study design, Setting, Patients, Intervention, Main outcome measures, Results and Conclusion หรือไม่
Background Risk of CV events is increased from 2- to 4-fold in type 2 diabetes Aspirin is recommended for primary prevention in patients with type 2 diabetes in many guidelines, including ADA
Background In subgroups with diabetes did not demonstrate a significant effecton reducing vascular events because they were underpowered. This trial was undertaken to examine the efficacy of low-dose aspirin therapy for the primary prevention of atherosclerotic events in patients with type 2 diabetes.
6 บทความดังกล่าวมีการอ้างอิงถึงบทความอื่นๆ ที่เป็นที่ยอมรับกันทั่วไปทางการแพทย์หรือไม่ และมีการอ้างอิงถึงบทความสำคัญเกี่ยวกับเรื่องดังกล่าวที่เพิ่งได้รับการตีพิมพ์ล่าสุดหรือไม่ • มีการอ้างอิงถึง Guideline ของ ADA 2003 ซึ่งแนะนำให้ใช้ aspirin เป็น primary prevention ในผู้ป่วยเบาหวานที่มีปัจจัยเสี่ยงต่อโรคหลอดเลือดหัวใจ และมีอีกหลาย Guideline ที่กล่าวถึงการใช้ aspirin เป็น primary prevention ในผู้ป่วยเบาหวานซึ่งตีพิมพ์ในปี 2002-2008
8 มีการกล่าวโดยย่อถึงผลการศึกษาที่ได้มีการดำเนินการศึกษามาก่อนหรือไม่ มีการกล่าวถึงสาเหตุของการจัดทำการศึกษาครั้งนี้หรือไม่ • มีการกล่าวถึงข้อจำกัดของการศึกษาก่อนหน้า ที่ให้ผลการศึกษาไม่แตกต่างกันระหว่างการใช้ low-dose aspirin ในการป้องกันการเกิด atherosclerosis เนื่องจากมี power ไม่เพียงพอ • สาเหตุของการจัดทำการศึกษาครั้งนี้ เนื่องจากหลาย Guideline แนะนำการใช้ aspirin เป็น primary และ secondary prevention ซึ่งข้อมูลการศึกษาทางคลินิกของการใช้ aspirin เป็น primary prevention ยังมีจำกัด
9 มีการกล่าวถึงสมมติฐานหรือวัตถุประสงค์ของการศึกษาอย่างชัดเจนหรือไม่ • วัตถุประสงค์ของการศึกษานี้คือ เพื่อศึกษาประสิทธิภาพของ low-dose aspirin ในการป้องกันการเกิด atherosclerosis ในผู้ป่วยเบาหวานชนิดที่ 2
Method Design: Prospective, randomized, open-label, controlled trial with blinded end point assessment 163 institutions in Japan from December 2002 to May 2005 with follow-up to April 2008 The institutional review board at each participating hospital approved this trial, and written informed consent was obtained from each patient.
Trial Population • Inclusion Criteria: Type 2 diabetes between ages 30 and 85 years • Exclusion Criteria: • electrocardiographic changes • a history of coronary heart disease confirmed by coronary angiography • a history of cerebrovascular disease • a history of arteriosclerotic disease • atrial fibrillation • pregnancy • use of antiplatelet or antithrombotic therapy, • a history of severe gastric or duodenal ulcer • severe renal and liver dysfunction • allergy to aspirin.
Trial Protocol • Enrolled patients were randomly assigned to the aspirin group (81 mg or 100 mg of aspirin OD) or the nonaspirin group by nonstratified randomization from a random number table. • Follow-up visits were scheduled every 2 weeks for patients seen in a clinic setting and every 4weeks for patients seen in a hospital setting. • Data for patients who were lost to follow-up were included at the day of last follow-up. • Patients in the non aspirin group were also allowed to use antiplatelet/thrombotic therapy, including aspirin, if needed.
End Points Primary end point: any atherosclerotic event death from coronary, cerebrovascular, and aortic causes nonfatal acute myocardial infarction unstable angina newly developed exertional angina nonfatal ischemic and hemorrhagic stroke transient ischemic attack nonfatal aortic and peripheral vascular disease Secondary end points: Each primary end point and combinations of primary end points and death from any cause Adverse events analyzed included gastrointestinal events and any hemorrhagic events other than hemorrhagic stroke
Sample size calculation • The incidence of cardiovascular death 7.5, myocardial infarction 7.5, and cerebrovascular events 8.0 events per 1000 patients-year (Hisayama-cho study and Funagata study). • The atherosclerotic events, including peripheral arterial disease, was suggested to be 3 times (HOT study). • Discounted 25% of the estimated 69 events that were expected to occur and estimated that 52 events per 1000 patients-year.
Sample size calculation • Based on a 2-sided α level of .05, a power of 0.95, an enrollment period of 2 years, and a follow-up period of 3 years after the last enrollment. • We estimated that 2450 patients would need to be enrolled to detect a 30% relative risk reduction for an occurrence of atherosclerotic disease by aspirin.
Statistical Analyses • Efficacy comparisons were performed on the basis of time to the first event, according to the intention-to-treat principle. • Safety analyses were performed on data from all enrolled patients. • Following the descriptive statistics, cumulative incidences of primary and secondary end points were estimated by the Kaplan-Meier method and differences between groups were assessed with the log-rank test. • We used the Cox proportional hazards model to estimate hazard ratios (HRs) of aspirin use along with 95% confidence intervals (CIs). • We used the x2 test or Fisher exact test to evaluate adverse events.
Statistical Analyses • We also conducted subgroup analyses for predetermined subgroups • Using the Cox proportional hazard model • P values of less than .05 were considered statistically significant.
5 สถานที่ที่ทำการศึกษาเหมาะสมหรือไม่ • เหมาะสม มีการทำใน 163 สถาบันที่แตกต่างกันในประเทศญี่ปุ่น ซึ่งมีความหลากหลาย ทำให้นำข้อมูลมาวิเคราะห์ได้อย่างครอบคลุม
10 รูปแบบของวิธีทำการศึกษา (Study design) เหมาะสมกับสมมติฐานหรือไม่ มีจริยธรรมหรือไม่ • เป็นการศึกษาแบบ Prospective, randomized, open-label, controlled trial with blinded end point assessment เหมาะสม เพราะการศึกษานี้เป็นการศึกษาประสิทธิภาพยา จึงควรศึกษาแบบ RCT • การศึกษานี้ให้ผู้ป่วยลงชื่อยินยอมเข้าร่วมการศึกษา และรับรู้ว่าตนเองอยู่ในกลุ่มการศึกษาใด
11 มีการกำหนดเกณฑ์โดยละเอียดของการคัดเลือกผู้เข้าร่วมการศึกษา การคัดออกจากการศึกษาหรือไม่ • มีการกำหนดการคัดเลือกเข้าร่วมและคัดออกดังนี้ • Inclusion Criteria: Type 2 diabetes between ages 30 and 85 years, and ability to provide informed comsent. • Exclusion Criteria: electrocardiographic changes consisting of ischemic ST-segment depression, ST-segment elevation, or pathologic Q waves; a history of coronary heart disease confirmed by coronary angiography; a history of cerebrovascular disease consisting of cerebral infarction, cerebral hemorrhage, subarachnoid hemorrhage, and transient ischemic attack; a history of arteriosclerotic disease necessitating medical treatment; atrial fibrillation; pregnancy; use of antiplatelet or antithrombotic therapy, defined as aspirin, ticlopidine, cilostazol, dipyridamole, trapidil, warfarin, and argatroban; a history of severe gastric or duodenal ulcer; severe liver dysfunction; severe renal dysfunction, and allergy to aspirin.
12 จำนวนของผู้เข้าร่วมการศึกษาเหมาะสมหรือไม่ สามารถเป็นตัวแทนของกลุ่มประชากรเป้าหมายได้หรือไม่ • จากการคำนวณขนาดตัวอย่าง พบว่าการศึกษานี้ต้องใช้จำนวนผู้ป่วย 2450 ราย • การศึกษานี้สามารถ enrolled ผู้ป่วยเข้ามาได้ 2539 ราย ถือว่ามีความเหมาะสมและเป็นตัวแทนของกลุ่มประชากรเป้าหมายได้
15 วิธีการเลือกตัวอย่างประชากรเป็นการสุ่มตัวอย่างที่แท้จริงหรือไม่ • Enrolled patients were randomly assigned to the aspirin group or the nonaspirin group by nonstratified randomization from a random number table. • The study center prepared the sealed envelopes with random assignments and distributed them by mail to the physicians in charge at the study sites.
16 ขนาดของการรักษา ความถี่ และระยะเวลาของการให้การรักษาเหมาะสมและเทียบเคียงในแต่ละกลุ่มหรือไม่ • กลุ่ม aspirin ได้รับ aspirin ขนาด 81 หรือ 100 mg วันละหนึ่งครั้ง ซึ่งตรงกับขนาดยาที่แนะนำใน ADA 2003 ซึ่งแนะนำการใช้ aspirin 81-325 mg ในผู้ป่วยเบาหวานที่มีความเสี่ยงสูงในการเกิดโรคหลอดเลือดหัวใจ • ผู้ป่วยได้รับยาตั้งแต่ 2002-2005 ซึ่งนานเพียงพอที่จะเห็นประสิทธิภาพของ aspirin ในการป้องกันการเกิด atherosclerosis และมีการติดตามผลการใช้ยาจนถึงปี 2008
17 ถ้าใช้บุคคลกลุ่มเดิมเป็นกลุ่มศึกษาและกลุ่มควบคุม ได้มีช่วงระยะเวลาพัก (Washout period) เพียงพอหรือไม่ • ผู้ป่วยในการศึกษานี้กลุ่มการศึกษาและกลุ่มควบคุมเป็นผู้ป่วยคนละกลุ่ม จึงไม่จำเป็นต้องมีช่วงระยะเวลาพัก (Washout period)
18 กลุ่มตัวอย่าง (กลุ่มตัวอย่างและกลุ่มควบคุม) สามารถรับประทานยาอื่นร่วมด้วยหรือไม่ มีการควบคุมเกี่ยวกับการได้รับยาชนิดอื่นหรือไม่ • กลุ่มตัวอย่างจำเป็นต้องได้รับยาอื่นร่วมด้วย เนื่องจากผู้ป่วยมีโรคประจำตัว ได้แก่ เบาหวานชนิดที่ 2 ความดันโลหิตสูง ไขมันในเลือดสูง
19 การศึกษาเป็นลักษณะปกปิด (เช่น single blind, double blind เป็นต้น) หรือไม่ • เป็นการศึกษาแบบ open-label แต่มีการปกปิดข้อมูลสำหรับผู้ทำการวิเคราะห์ข้อมูล (blinded end-point assessment)
20 ถ้ามีผู้สังเกตการณ์ คุณสมบัติของผู้สังเกตการณ์มีความเหมาะสมหรือไม่ มีการใช้เทคนิคการปกปิด (blind technique) กับผู้สังเกตการณ์หรือไม่ • บทความไม่ได้แสดงข้อมูลผู้สังเกตการณ์ • มีการปกปิดข้อมูลสำหรับผู้ทำการวิเคราะห์ข้อมูล (blinded end-point assessment)
21 มีวิธีวัดถึงประสิทธิผลของการรักษาหรือไม่ • วิธีวัดประสิทธิผลของการรักษาในการศึกษานี้คือ อุบัติการณ์ของ atherosclerotic events และอาการไม่พึงประสงค์จากการใช้ยา Primary end point: any atherosclerotic event Secondary end points: Each primary end point and combinations of primary end points and death from any cause Adverse events analyzed included gastrointestinal events and any hemorrhagic events other than hemorrhagic stroke
22 วิธีชี้วัดเป็นการประเมินทาง subjective หรือ objective หรือไม่ • วิธีชี้วัดเป็นการประเมินทาง Objective ได้แก่ การเกิด atherosclerotic events
23 ความเชื่อถือได้ ความจำเพาะเจาะจง หรือความเชื่อถือได้ทางวิธีชี้วัดเป็นอย่างไร ควรมีการใช้วิธีการอื่นที่สามารถเชื่อถือได้มากกว่าหรือไม่ • การเกิด atherosclerotic events เป็นการวัดที่น่าเชื่อถือ และเหมาะสมกับการศึกษาประสิทธิภาพของยาในการป้องกันโรค
24 มีการติดตามผลการรักษานานเท่าใด นานเพียงพอหรือไม่ • มีการให้ aspirin 2002-2005 และติดตามจนกระทั่งปี 2008 นานเพียงพอที่จะเห็นประสิทธิภาพยาในการป้องกันโรค
28 วิธีวิเคราะห์ทางสถิติที่ใช้เหมาะสมหรือไม่ • สถิติที่ใช้มีความเหมาะสม ดังที่กล่าวมาแล้วข้างต้น
Results • Study population • Baseline clinical characteristics • Efficacy analysis • Subgroup analysis • Safety
Study population 2567Patients were screened 28 Excluded 6 Withdrew consent 10 History of atherosclerotic disease 10 Aged >85 years 1 No diabetes 1 Receiving warfarin 2539 Randomized 1262 Randomized toreceive aspirin 1277 Randomized to nonaspirin group 1139 Received aspirin through completion of trial 123 Stopped taking aspirin 9 Received aspirin or other antiplatelet therapy 6 Received aspirin 3 Received other antiplatelet medication 1165 Followed up through end of study 97 Lost to follow-up 1181 Followed up through end of study 96 Lost to follow-up 1262 Included in efficacy and safety analyses 1277 Included in efficacy and safety analyses
Baseline Clinical Characteristics Baseline Clinical Characteristics
13 ลักษณะต่างๆ ของกลุ่มศึกษา (เช่น ช่วงอายุ เพศ ความรุนแรงของโรค เป็นต้น) มีการแจกแจงอย่างเหมาะสมหรือไม่ และถ้ามีกลุ่มควบคุม ลักษณะต่างๆ ขั้นต้น มีความแตกต่างจากกลุ่มการศึกษาอย่างมีนัยสำคัญทางสถิติหรือไม่ • มีการแจกแจงลักษณะของกลุ่มตัวอย่างเหมาะสม แต่ไม่มีการแสดงค่าทางสถิติที่บ่งบอกถึงความแตกต่างระหว่างกลุ่มตัวอย่าง
14 กลุ่มควบคุมมีคุณสมบัติเหมาะสมหรือไม่ • เนื่องจากไม่มีการแสดงค่าทางสถิติที่บ่งบอกถึงความแตกต่างระหว่างกลุ่มตัวอย่าง จึงไม่สามารถประเมินความเหมาะสมของกลุ่มควบคุมได้
Primary End Point: Total Atherosclerotic Events According to the Treatment Groups 1262 1210 1159 1095 806 140 Aspirin Group (n) 1277 1220 1165 1117 813 135 Nonaspirin Group (n) 10 8 Log-Rank Test, P = 0.16 HR (95% CI): 0.80 (0.58–1.10) 6 % 4 Aspirin Group Nonaspirin Group 2 0 Years 0 1 2 3 4 5
Subgroup Analysis Events, No./Total No. Favors No Aspirin Favors Aspirin 2.0 1.0 0.3 Hazard Ratio (95% CI)