Download
1 / 23
230 likes | 278 Vues
Utility of Total Serum IgE in Allergy. Anne Barasa, MBChB, MMed (Path ) Lecturer, Immunology Unit Department of Human Pathology University of Nairobi KPA 2019. Immunoglobulin E. 5 th Immunoglobulin class

E N D
Utility of Total Serum IgE in Allergy Anne Barasa, MBChB, MMed (Path) Lecturer, Immunology Unit Department of Human Pathology University of Nairobi KPA 2019 University of Nairobi ISO 9001:2008 1 Certified http://www.uonbi.ac.ke
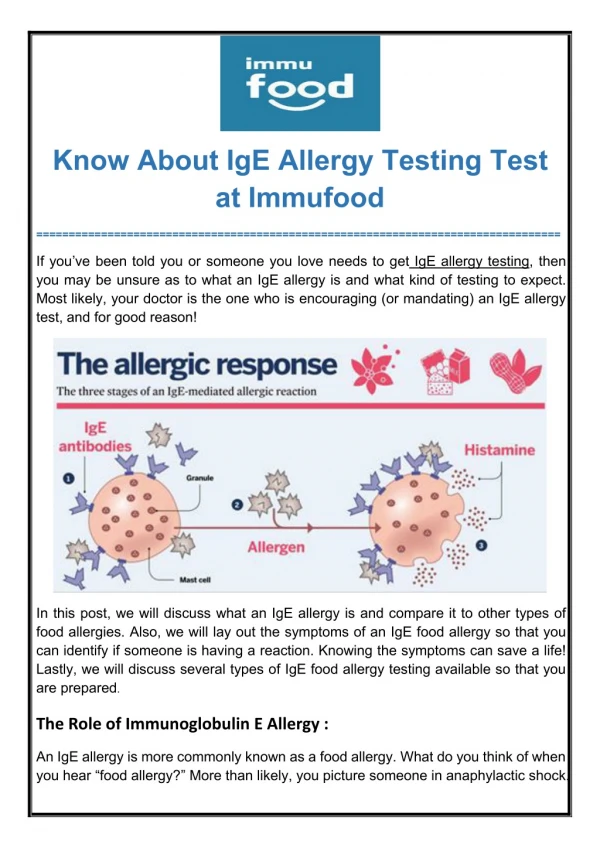
Immunoglobulin E • 5th Immunoglobulin class • Once produced, IgE binds to its receptors, through which it mediates its functions • High-affinity receptors (FcεRI) - mast cells, basophils, APCs • Low-affinity receptors (FcεRII/CD23) – B cells, monocytes, dendritic cells • Present in serum in small quantities (0.0005% of total immunoglobulin) • In equilibrium with that which is cell-bound
Role of IgE in Health and Disease • Physiological role – defense against parasites • Helminths • Protozoa • Pathological - Type I hypersensitivity reactions
Pathogenesis of Allergy • Re-exposure • Binding of allergen to IgE-FcεRI complexes cross-links the receptors, leading to cellular activation • Degranulation & mediator release (histamine) • Synthesis of lipid mediators (prostaglandins, leukotrienes) • Synthesis of cytokines (IL-4, -5) Sensitization
Serum levels of Total IgE • Age-dependent • Progressive increase in healthy children, up to age 10 – 15 years • Increase in atopic children is earlier and steeper • Gradual decline from 2nd decade of life • Should always be evaluated to the reference intervals established from age-stratified healthy (non-atopic) populations
Serum levels of Total IgE • Serum levels also influenced by • Race • Gender • Geographic area • Season • Exposure to environmental pollutants • Non-allergic diseases • These make determination of reference ranges difficult • Clinical utility dependent on establishment of reliable reference values for the respective population
IgE Levels in Populations in the Tropics • High serum levels of tIgE in people living in helminth endemic areas of the tropics, despite being non-atopic • Helminths capable of inducing IgE synthesis markedly • Mostly non-specific IgE • Postulated that polyclonal IgE synthesis is a mechanism of the parasite to evade the host immune response against it
Causes of Elevated Serum tIgE • Allergic disease • Levels significantly higher in atopic disorders than age-adjusted healthy populations • Significantly increased in parasitic infections (helminths)
Causes of Elevated Serum tIgE • Non-parasitic infections (EBV, CMV, HIV, M.Tb) • Inflammatory diseases (Vasculitides) • PIDs (Hyper IgE, Wiskott-Aldrich syndrome) • Malignancies (Hodgkins lymphoma, IgE myeloma)
Diagnostic Performance • i.e.. Ability to detect aetiology • Expressed as clinical sensitivity and specificity • Based on a given cut-off value, below which the test is considered negative, and above which it is considered positive • Raising the cut-off makes the test more specific but less sensitive; and vice-versa
Limited diagnostic value of tIgE despite many patients with allergic disorders having elevated levels
Insufficient diagnostic accuracy of tIgE levels alone to detect allergic diseases, regardless of cut-off used 77.7 kU/L – optimal cut-off on ROC curve 164.3 kU/L – upper 95% CI in non-atopic children 100 kU/L – commonly used cut-off in clinical practice
Clinical Utility of tIgE for Allergy • Commonly requested test as first line test to clarify a state of sensitization, as a risk factor for allergic disease • Higher levels of tIgE in patients with allergic diseases compared with non-allergic patients • Does not prove existence of an allergic disease state • As many as 5% of healthy children may have serum tIgE concentrations above the age-specific reference range • 10% children with clinical signs of hypersensitivity may have serum tIgE concentrations within the age-specific reference range (Some studies report up to 33%)
Clinical Utility • Necessitated identification of cut-off levels to aid in diagnosis of allergy • Cut-off of >200 kU/L proposed to have high probability in predicting presence of sensitization/allergy
Positive sIgE findings found in 8% study subjects • Total IgE values below 10 kU/L do not exclude the presence of sensitization • Recommended that sIgE concentrations should be determined in children with low tIgE values in cases of clinically suspect allergic reactions
Clinical Utility - Limitations • Considerable overlap in serum tIgE levels between atopic and non-atopic populations reduces its utility in identifying atopy • Detects total amount of IgE present in blood, irrespective of what these IgE molecules bind to • Need to distinguish allergen-specific vs non-allergen-specific IgE
Clinical Utility in Allergy • Supplemental diagnostic measure for the diagnosis of allergic asthma (Szefler SJ et al, Asthma outcomes: biomarkers; Journal of Allergy and Clinical Immunology; 2012) • Evaluation of candidates for anti-IgE therapy
Clinical Governance and Value-Based Care • Lab medicine practitioners take responsibility to ensure cost effective use of lab tests • In children in whom allergy might be suspected but no definite clues exist to explain vague symptoms, a battery of tests (tIgE and sIgE) not recommended • The practice of “over use” of blood screening tests not recommended Sinclair D, Peters SA; J Clin Pathol 2004
Clinical Governance and Value-Based Care • Clinical justification of the test based on careful history and physical examination • Total IgE should not be used as a screen for subsequent testing • If the clinical history is of a convincing allergic reaction, a low total IgE does not preclude the presence of allergen sIgE • With a history of an acute reaction, proceed with clinically appropriate allergen sIgE tests Sinclair D, Peters SA; J Clin Pathol 2004
Conclusions • Elevated serum IgE can be detected in subjects sensitized to allergens, as well as in non-allergic diseases • Measurement of total IgE (and then allergen sIgE if the level is above a certain cut-off) has relatively low levels of sensitivity and specificity • High total IgE levels do not indicate an allergy • Normal levels do not necessarily indicate absence of allergy
Conclusions • Serum tIgE testing for allergy is non-specific; does not give information on sensitizing allergens • Therefore of limited clinical utility as a screen or diagnostic test for allergic disorders • Replaced by more specific and sensitive markers (sIgE; component resolved diagnostics)
Recommendations • Comprehensive atopic history of the patients • Proper selection and interpretation of specific IgE testing • Interpretation within clinical context