Case study 4
Explore the approach, evaluation, diagnosis, and treatment of acute psychosis in a 79-year-old Thai male patient presenting with delusions and hallucinations.

Case study 4
E N D
Presentation Transcript
Case study 4 Ext.ปานเกล้า ศิริอาชาวัฒนา
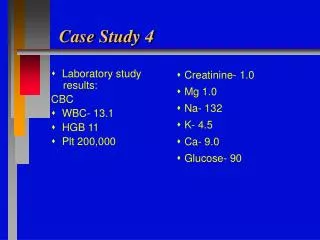
Case 4 • Case ผู้ป่วยชายไทย อายุ 79 ปี ญาตินำส่งโรงพยาบาลด้วยอาการเพ้อ สับสน ประมาณ 2 วันก่อนมาโรงพยาบาล ผู้ป่วยมีเห็นภาพหลอน กลัวผีจะมาทำร้าย พูดเพ้อคนเดียว ไม่รู้วัน เวลา สถานที่ นอนไม่หลับ กินข้าวไม่ได้ (ไม่ยอมกินข้าว) อ่อนเพลีย ไม่มีแรง ผู้ป่วยไม่เคยมีอาการอย่างนี้มาก่อน • V/S BT 38.5˚c, BP 110/70, RR 20, PR 80, ท่านเป็นแพทย์เวรที่ ER
Problem listของผู้ป่วยรายนี้คืออะไรบ้าง
Approach • Always consider medical disorders esp. if no previous psych HX • Anticipate need for psychiatry consult and restraints (meds, physical) early
Problem list • Old patient: 79 years-old • Psychosis for 2 days: delusion, hallucinations, bizarre behavior, disorganized speech • Fever: BT 38.5˚c
ท่านจะซักประวัติเพิ่มเติมอะไรบ้างท่านจะซักประวัติเพิ่มเติมอะไรบ้าง
History • Ask open-ended ?’s re: thoughts, feelings, personal relationships; drug use; prior hospitalizations/psych hx; psychiatric medications; physical/sexual abuse • Psychosis: delusion, hallucinations, bizarre behavior, disorganized speech
Findings • Abnormal vital signs; appearance, mental status exam • Head-to-toe exam: E/O trauma, pupils, nystagmus, thyroid, pulm/cardia/abdomen, skin • Neuro: CNs, DTRs, motor, sensory, cerebellar, asterixis, gait, catatonia (consider NMS)
ท่านจะส่งLab investigation เพิ่มเติมอะไรบ้าง
Evaluation • Consider ECG and psych med levels (ie, Li) • Tox: if concern for unreported drug abuse or ingestion (id, acetaminophen) • Psychiatry consult: if ? Need for hospitaliz, suicide/homicide attempt, uncertain @ risk of danger to self/other
Evaluation • Other labs: if concern for “organic” d/o or required for psychiatric hospital: CBC, chem7, LFTs, UA, TSH, ammonia, CXR • More thorough w/u is necessary for new onset psychiatric dx: consider RPR, CT head, LP, EEG
จงให้การวินิจฉัยผู้ป่วยรายนี้จงให้การวินิจฉัยผู้ป่วยรายนี้
Diagnosis • Acute Psychosis due to medical disorder
จงให้การวินิจฉัยแยกโรคผู้ป่วยรายนี้จงให้การวินิจฉัยแยกโรคผู้ป่วยรายนี้
จงให้การ managementผู้ป่วยรายนี้
Treatment • Treat any underlying medical illness • Meds • Haldol (IM/IV), loanzapine (PO/SL/IM); side effects; QT, akathisia, dystonia • Lorazepam/diazepam (PO/SL/IM): preferred for drug-related agitation; avoid in the elderly
Treatment • Physical restraints: soft/leather (1-4 points), posy: use as temporizing measure in conjunction with pharmacologic treatment and 1:1 sitter
Pearls • Signs suggestive of “organic disorder” age > 40 w/ no prior psych hx, abnl VS, recent memory loss, clouded consciousness • Engage family member/friends/partners whenever possible