A-V pattern Horizontal strabismus
A-V pattern Horizontal strabismus. A R Zandi Feiz hospital. Change in magnitude of deviation in upgaze and downgaze. A-V pattern is a vertical incomittancy. A pattern. More convergent in upgaze compared with downgaze. V pattern. More convergent in downgaze compared with upgaze.

A-V pattern Horizontal strabismus
E N D
Presentation Transcript
A-V patternHorizontal strabismus A R Zandi Feiz hospital
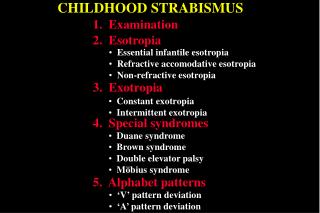
A pattern • More convergent in upgaze compared with downgaze
V pattern • More convergent in downgaze compared with upgaze
An A or V pattern is found in 15%-25% of horizontal strabismus
Cause • Bilateral oblique muscle dysfunction
These associations reflect the ancillary abducting action in upgaze and downgaze
Cause…. • Horizontal rectus muscle dysfunction
Cause…. • Vertical rectus muscle dysfunction
Clinical features • Measurement of the alignment in downgaze and upgaze
When in 25` from the primary position at least 10^ difference in deviation is detected, the clinically significant A pattern is present
To be a clinically significant V pattern the difference must be at least 15^
Management • Surgery for= Clinically significant pattern
Surgery for pattern • Most often in combination with correction of the underlying horizontal deviation
Patients with large A or V pattern usually also have significant corresponding oblique muscle dysfunction
If the pattern is related to overaction of the oblique muscle,these are weakened as part of the surgical plan
Weakening the IO muscles or tucking the SO tendons corrects up to 15-25^ of V pattern
Bilateral SO tenotomy correct up to 35-45^ of A pattern(they produce 35-45^ esoshift in downgaze)
Displacing the horizontal rectus muscle insertions is indicated when there is no oblique dysfunction
The amount of displacement usually is ½ to a full tendon width
MR are always moved toward the direction where convergence is greater or divergence is less(upward in A pattern and downward in V pattern)
This displacement has no net horizontal,vertical or torsional effect in the primary position
For example for V pattern when MR is displaced downward(and LR upward) in downgaze MR will be relaxed and the LR will be tightened( thereby decreasing the V pattern)
The muscle is moved in the direction in which the muscle`s horizontal effect is to be lessened