Understanding Progressive Muscular Dystrophy: Symptoms, Tests, and Nursing Interventions
Progressive Muscular Dystrophy refers to hereditary diseases affecting muscle strength and function. Learn about symptoms, tests, and nursing care for MD patients. Associated with various theories and issues like walking problems and muscle weakness.

Understanding Progressive Muscular Dystrophy: Symptoms, Tests, and Nursing Interventions
E N D
Presentation Transcript
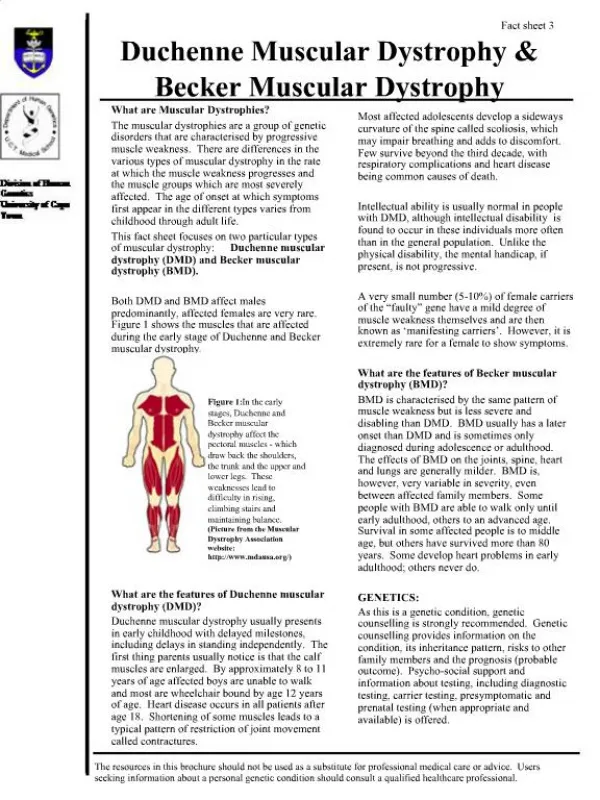
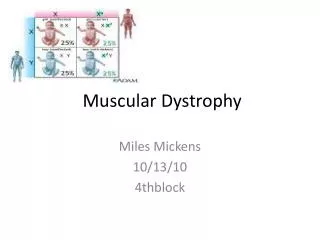
Muscular Dystrophy Definition Refers to a group of hereditary progressive diseases. Muscular Dystrophy affects muscular strength and action, some of which first become obvious in infancy, and others which develop in adolescence or young adulthood. The syndromes are marked by either generalized or localized muscle weakness, difficulties with walking or maintaining posture, muscle spasms, and in some instances, neurological, behavioral, cardiac, or other functional limitations.
Pathophysiologic the exact mechanism is unknown, but there are 3 theories • Vascular theory: the lack of blood flow causes the typical degeneration of muscle tissue. • Neurogenic theory: Disturbance in nerve-muscle interaction. • Membrane theory: the cell membranes are genetically altered, causing a compromise in cell integrity. An increase in the activity of muscle proteolytic enzymes may accompany the membrane alteration. Leaving the muscle cell vulnerable to degeneration.
Symptoms • Muscle weakness • Delayed development of muscle motor skills • Problems walking (delayed walking) • Difficulty using one or more muscle groups (depends on the type of dystrophy) • Eyelid drooping (ptosis) • Drooling • Hypotonia • Mental retardation ( only present in some types of MD) • Joint contractures (clubfoot, clawhand or others) • Scoliosis
Signs and Tests Examination and history help to distinguish the type of MD. Specific muscle groups are affected by different types of MD. Often, there is a loss of muscle mass (wasting), which may be disguised in some types of muscular dystrophy by an accumulation of fat and connective tissuethat makes the muscle appear larger (pseudohypertrophy).Joint contractures are common. Shortening of the muscle fibers, fibrosis of the connective tissue and scarring slowly destroy muscle function. Some types of MD involve the heart muscle, causing cardiomyopathy or arrhythmias.A muscle biopsy may be the primary test used to confirm the diagnosis. In some cases a DNA test from the blood may be sufficient.
Laboratory Test Muscle biopsy: the primary test used to confirm the diagnosis. DNA test Serum CPK (creatine phosphokinase-an enzyme found in muscle) may be elevated. EMG (electromyography) may confirm that weakness is caused by destruction of muscle tissue rather than damage to nerves. ECG (electrocardiography) to monitor changes in cardiac status. Myoglobin - urine/ serum: When muscle is damaged, the myoglobin is released into the bloodstream. It is filtered out of the bloodstream by the kidneys, and eliminated in urine. In large quantities, myoglobin can damage the kidney and break down into toxic compounds, causing kidney failure. LDH: LDH is most often measured to evaluate the presence of tissue damage. The enzyme LDH is in many body tissues, especially the heart, liver, kidney, skeletal muscle, brain, blood cells, and lungs. Creatinine : A normal (usual) value is 0.8 to 1.4 mg/dl. Creatinine is a breakdown product of creatine, which is an important constituent of muscle. A serum creatinine test measures the amount of creatinine in the blood. Greater-than-normal levels may indicate: Muscular dystrophy. Lower-than-normal levels may indicate: Muscular dystrophy (late stage) AST: The normal range is 10 to 34 IU/L. An increase has many indications, one of them being progressive MD. Aldolase: Why the test is performed? This test is indicator ofmuscle damage.
Nursing Diagnosis Impaired mobility, activity intolerance, risk for injury, risk for aspiration, risk for impaired skin integrity, self-care deficit, knowledge deficit, caregiver role strain, low self-esteem, social isolation, disturbed body image, and hopeless to name a few.
Nursing Implications and interventions: • Multidisciplinary. Care for these patients involves arranging for consultations with physical therapy, occupational therapy, respiratory therapy, speech therapy, psychosocial therapy, and dieticians. • Reinforce techniques learned in all of the above therapies. • Educate client and family members thoroughly about expected outcomes and possible problems. • Encourage exercise while teaching s/s of exercise overload: feeling weaker rather than stronger after exercise, excessive muscle soreness, severe muscle cramping, heaviness of extremities, and prolonged shortness of breath. • Ensure braces are a good fit to prevent pressure ulcers and promote stability. • Have equipment (braces, wheelchairs) evaluated by PT, OT to ensure proper fit. • Be sensitive to psychosocial needs and make appropriate referrals. • Refer to support groups and clinics.
Bibliography • Cart, Greg. “Rehabilitation Management of Neuromuscular Disease.” http://www.emedicine.com/pmr/topic233.htm. • Cox, Helen C., RN, C, EdD, FAAN. Clinical Applications of Nursing Diagnosis. 4th Edition. F.A. Davis Company. Philadelphia, PA: 2002. • Ignatavicius, Donna, MS, RN, CM. Medical-Surgical Nursing. 4th Edition. W.B. Saunders Company. Philadelphia, PA: 2002. • Muscular Dystrophy Association website: http://www.mdausa.org. • Harrison’s Principles of internal Medicine 15th edition, McGraw-Hill Medical Publishing Division, New York. 2002.