Intermediary Liners and Bases for Pulpal Protection in Restorative Dentistry
510 likes | 1.06k Vues
Learn about cavity liners and insulating bases used to protect the pulp and improve restoration outcomes in dentistry. Understand ideal material requirements, types, functions, and manipulation techniques.

Intermediary Liners and Bases for Pulpal Protection in Restorative Dentistry
E N D
Presentation Transcript
Intermediary Liners and Bases Presented By Dr. Somaya Ali
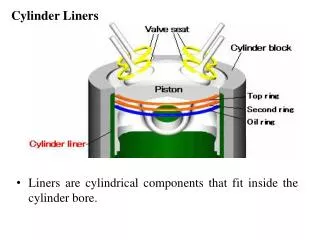
Cavity liners and insulating bases are materials placed between dentin (sometimes pulp) and restorative material to provide pulpal protection or pulpal response.
Pulpal protection: 1- Chemical protection. 2- Electrical protection. 3- Mechanical protection. 4- Biological protection. 5- Thermal protection.
Ideal requirements for intermediary materials: 1- It should provide no further irritation, be biocompatiblewith pulp-dentin organ and stimulate reparative dentin formation. 2- The material should provide a sedative and palliativeaction to the pulp.
Ideal requirements for intermediary materials: 3- It should improve the marginal sealingand the adaptation to the cavity walls. 4- The material should possess thermal and electrical insulating capacity
Ideal requirements for intermediary materials: 5- The material should have sufficient strengthto resist fracture or distortion under the forces of condensation of the permanent restoration and subsequent masticatory forces.
Ideal requirements for intermediary materials: 6- It should be compatiblewith overlying restorative material and other intermediary base materials. 7- The material should resistdegradationin the oral fluids. 8- It should have adequate workabilityand be easy to apply.
Cavity Varnish: It is supplied in the form of a liquid composed of 10% natural gum (copal or rosin) or synthetic resindissolved in 90% organic solvent such as ether, acetone or chloroform.
Cavity Varnish: - Functions. • Indications. • Contraindication.
Cavity Varnish: - Manipulation:
Dentin sealer. • Ex. Gluma desensitizer • Dentin bonding agents (DBAs).
Cavity Liners: • Calcium hydroxide: • Powder & liquid. • Suspension. • Paste-paste system. • One paste system
Reinforced ZnO & E • Multiple pharmacological actions. • Eugenol produces palliative,sedativeand obtundant action on the pulp when used in very low concentrations. • ZOE also has an antiseptic and anti-inflammatory effect. • ZOE can be placed in moderatelydeepcavities, when remaining dentin thickness is as low as 1mm.
Reinforced ZnO & E • It is an excellent thermal insulatorin a film thickness as low as 0.25mm. • It is an excellent electrical insulatorand has a good sealing ability. • Low strength properties and not rigid enoughto be used as a base. Despite improved strength properties of RZOE, it is still inferior to that of other cements.
Indications: • as a liner in moderately deep cavities to enhance pulpal healing. • As a temporaryfilling material and for temporarycementation. • As a basematerial, when biological consideration is more important than mechanical one.
Contraindications: • Very deep cavities(dentin bridge ≤ 0.5mm) or as a direct pulp capping material. • With resinous tooth colored restoratives (composite resin), as eugenol interferes with the setting reaction of any polymer and can even depolymerize already set polymeric materials. • With glass ionomer cementsas well as polycarboxylate cement, where it would deprive the bonding capabilities of these materials.
Glass ionomer cements: • It has an excellent sealing ability due to chemical adhesionto tooth structure through carboxylate ions released from PAA liquid. • It has an anticariogenic property due to fluoride release from the powder glass component.
Glass ionomer cements: • It is biocompatible with P-D organ and all permanent restorative materials. However, if remaining dentin thickness is less than 1mm protection of the pulp by a layer of Ca(OH) liner is needed. • It provides adequate thermal, chemical and mechanical protection as well as proper sealing of dentinal tubules. It is thus an excellent material to be used as dentin substitute.
Glass ionomer cements Advantages of RMGI over conv. GIC: • Flexible working time. • Improved strength and wear properties. • Ease of handling. However, conv. GIC has higher fluoride release especially during the first 24 hours (initial fluoride burst).
Glass ionomer cements: Indications: 1- sandwich technique 2- liner/base
Zinc polycarboxylate cement: PRESENTATION White powder zinc oxide with up to 10% magnesium oxide Clear Liquid 30-40% aqueous solution of polyacrylic acid
Properties and functions: • It bonds chemically to tooth structure, which leads to proper chemical protection as well as decreased microleakage. • The pH of the cement liquid is 1.7. In spite of its initial acidic nature, it produces minimal irritationto P-D organ. This is probably due to:
Properties and functions: • High biocompatibility.. Due to: • The pH of the mixed setting cement rises rapidly to 3.4 after two minutes from the start of mixing. • Polyacrylic acid is weaker than phosphoric acid. • Polyacrylic acid has low diffusion mobility into the underlying dentin due to its large molecular size and because of immediate complexing with fluoride and calcium of tooth structure which would hinder further penetration of the acid.
Properties and functions: • lower compressive strengththan ZPC, but significantly higher tensile strength. It provides proper mechanical protection. • It is a good thermal insulatorin thickness not less than 1.5 mm. It is also an electrical insulator. • It is compatiblewith all permanent restorative materials. It is compatible with other intermediary materials with the exception of ZOE and varnish…?
Zinc polycarboxylate cement: • Indications: It is used as a base under any restorative material and as luting cement.
Biodentine: • Bioactive Dentine Substitute • In September 2010 by Septodont. • Preservation of pulp vitality. • Prevention of clinical failures. • Ultimate dentin substitute.
Biodentine: Composition: Powder: • Tricalcium silicate, dicalcium silicate (core), calcium carbonate, oxide (filler), iron oxide (shade), and zirconium oxide (radiopacifier). Liquid: • calcium chloride (accelerator) and hydrosoluble polymer (water reducing agent) and water.
Biodentine: Setting Reaction: • CSH gel acts as a matrix of the cement with the crystals of CaCO3 are filling the spaces between the gel forming particles of the matrix. • Calcite (CaCO3 ) acts as an active agent implicated in the reaction and as a filler (improves the prop. Of the cement). • Final Hydration Reaction includes unreacted CS particles, CSH gel and Ca(OH)2 .
Biodentine: Setting Reaction: • C3S + H2O CSH + Ca(OH)2 • Mixing time 30 sec. in amalgamator.
Biodentine: Properties: • Setting Time: • 45 min. (9-12 min initial setting). • Adhesion: • Crystal growth within dentinal tubules …….. Long lasting seal. • Ion exchange with dentine. • Density and porosity: • Hydrosol polymers … decrease amount of water ….. Improve density ….. Better mechanical prop.
Biodentine: Properties: • Radiopacity: • Due to zirconium oxide…. Better to be identified in radiographs. • Compressive strength: • More than 200 Mpa at first 24 Hrs. • Improves up to 300 Mpa within one month approaching that of natural dentine (297 Mpa). • Biodentine – Tooth interface: • ppt of apatite like Ca-Phosphate crystals….high acid erosion and microleakage resistance .
Biodentine: Properties: • Ion Release: • Ability to release Ca and OH ions. • Antibacterial properties: • CaOH ions released …… increase pH to 12. • Stability in the oral fluids: • Not as stable as composite restorations….so? • More stable than other comparable materials.
Biodentine: • Minimal P.reaction. • High biocompatibility • Low risk of P tissue reaction. • Bioactive properties. • Stimulate 2ry D formation (lasts for 3 months). • Pulp healing promotion. • Deep cavities. • Pulp Capping (Direct/Indirect).
Biodentine: • Prevention of clinical failures. • Mineral tags in DT. • High dimensional stability. • Low risk of bacterial percolation. • Remineralization of interfacial D. • No conditioning or bonding. • Natural micro-mechanical anchorage in DT and ion exchange chemical bonding. • Full restoration in one session. • Low chair time
Theracal: • A light cured, resin modified calcium silicate filled liner. • Designed for use in direct and indirect pulp capping, as a protective base/liner under composites, amalgams, cements, and other base materials. • Performs as an insulator/barrier and protectant of the dental pulpal complex
Theracal: • Consists of tricalcium silicate particles in a hydrophilic monomer (significant calcium release making it a uniquely stable and durable material as a liner or base). • Calcium release stimulates hydroxy-apatite and secondary dentin bridge formation
Theracal: • May be placed directly on pulpal exposures after hemostasis is obtained. It is indicated for any pulpal exposures. • Has the capability to be cured to a depth of 1.7 mm (no risk of untimely dissolution)….. Major advantages in direct pulp capping treatments.
Clinical judgment for the need of a specific liner or base material depends mainly on: 1-Remaining dentin thickness (RDT); as the depth of the cavity increases, the RDT decreases and there is more need for intermediary materials before inserting the permanent restoration.
Clinical judgment for the need of a specific liner or base material depends mainly on: 2-Adhesive properties of liner or base; to benefit from its adhesive potential, an intermediary material should be placed directly on tooth structure except where pulpal medication is essential.
Clinical judgment for the need of a specific liner or base material depends mainly on: • 3-Type of restorative material; whether is a metallic or adhesive esthetic restoration, a direct or indirect one.