Atrial Flutter
Atrial Flutter. Chris Caulfield AM Report 2/19/10. Definition. Atrial Flutter is rapid, regular atrial depolarizations at a characteristic rate of approximately 300 beats/min.

Atrial Flutter
E N D
Presentation Transcript
Atrial Flutter Chris Caulfield AM Report 2/19/10
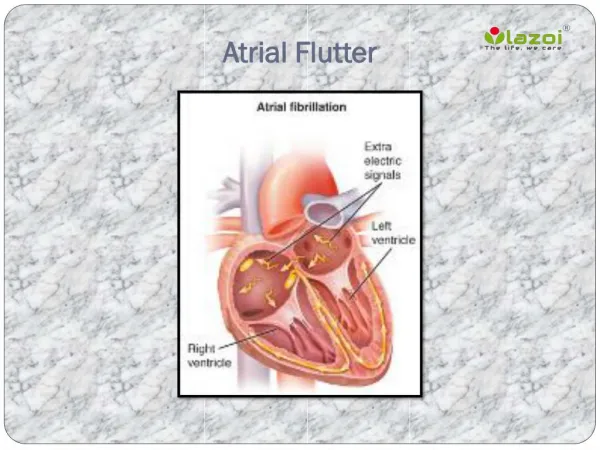
Definition • Atrial Flutter is rapid, regular atrial depolarizations at a characteristic rate of approximately 300 beats/min. • Prolonged atrial flutter can ultimately impair cardiac output, increase myocardial oxygen demand, and cause atrial thrombus formation.
Epidemiology • In one study, estimated that the incidence of in the United States is about 200,000 new cases per year, and occurs more common in men and in older adults. • Risk of developing atrial flutter increased 3.5 times in patients with heart failure and 1.9 times in those with chronic obstructive lung disease • Unusual to occur in a normal heart, and is especially uncommon in children and young adults
Classification of Type • Type I is considered typical and has an atrial rate 240 to 340 beats/min • Type II is considered atypical and has an atrial rate of 340 to 440 beats/min
Type I Atrial Flutter • Typical atrial flutter, or "isthmus-dependent" flutter, is a macroreentrant arrhythmia that involves a long slow path with an excitable gap, forming a circuit within the right atrium. • Slowly conducting reentrant circuit is located in the low right atrial isthmus. • The isthmus of tissue is between the inferior vena cava and tricuspid annulus.
Type II Atrial Flutter • Atypical atrial flutter lacks an excitable gap and is not isthmus-dependent. • Usually this rhythm results from an intra-atrial reentrant circuit that is very short. • May be due abnormal anatomy within the right or left atrium (i.e. surgical scars, irregular pulmonary veins, disturbed mitral annulus)
Symptoms • Palpitations • Fatigue • Lightheadedness • Shortness of breath • Less common symptoms include angina, hypotension, or syncope
Diagnosis: EKG • EKG will typically show 2:1 conduction across the AV node (even ratios of conduction are more common than odd ratios) • 1:1 conductive response suggests catecholamine excess, parasympathetic withdrawal, or the existence of an accessory bypass tract in pre-excitation • May need to administer adenosine to slow conduction through AV node
Rheumatic heart disease (if MV involved) LV dysfunction/heart failure Sick sinus syndrome Pericarditis Pulmonary embolism Chronic obstructive pulmonary disease Mitral valve prolapse Hyperthyroidism Status post CABG Diagnosis: Underlying Causes • Uncommon complication of acute MI and digitalis toxicity
Further Diagnosis • Serum electrolytes, pulmonary and thyroid function tests should be ordered if appropriate. • Transthoracic echocardiography should be performed to evaluate for structural and valvular abnormalities along with LV systolic function. • Holter monitoring or event recorders could be provided in an ambulatory setting if symptoms are non-specific and an arrhythmia is considered but has not been detected. • Electrophysiological studies may be required at a later point for further diagnosis and therapy.
Treatment • Control of ventricular rate • Reversion to NSR • Maintenance of NSR • Prevention of systemic embolization
Control of ventricular rate • Intravenous calcium channel blockers (Diltiazem or Verapamil) or beta blockers (Esmolol) may be used to control rapid ventricular rate. • Digoxin is not typically used except occasionally in patients with heart failure. • Amiodarone can also be used for control of rapid ventricular response, but could promote conversion to sinus rhythm, increasing risk of embolization if not anticoagulated.
Reversion to NSR • The optimal outcome of atrial flutter is reversion to and maintenance of normal sinus rhythm, not ventricular rate control. • Cardioversion can be performed by electrical or chemical means. • DC cardioversion is the choice for reversion to sinus rhythm if the patient is hemodynamically unstable and is uninstrumented. (starting at 50 to 100 J with biphasic defibrillators) • Stable patients may convert after watchful waiting. • Factors that predict spontaneous reversion to sinus rhythm or a successful cardioversion include: • Left atrial size less than 4.5 to 5 cm • Atrial flutter of recent onset with little or no heart failure • No underlying reversible cause (i.e. hyperthyroidism)
Chemical Cardioversion • Anti-arrhythmic agents that can be used for cardioversion include flecainide, dofetilide, propafenone, ibutilide, and amiodarone. • Flecainide is contraindicated in CAD, structural heart disease, and LVH (as per CAST) • LV hypertrophy without ischemia or conduction delay, class III agents, specifically amiodarone, can be used. • Ischemic heart disease, sotalol or amiodarone can be used. (Avoid class IC agents) • Significant systolic dysfunction, amiodarone and dofetilide can be used. (Avoid class IC agents) • Slowing of the atrial flutter rate with anti-arrhythmics alone can lead to 1:1 conduction. • Class IA and IC drugs should be administered in conjunction with an AV nodal blocking agent (beta blocker or calcium channel blocker)
Anticoagulation • It is unusual to have thrombus form in the left atrial appendage because of the regularity of atrial contractions in atrial flutter. • However, atrial fibrillation can be a rhythm underlying atrial flutter. • As in Afib, if atrial flutter persists for more than 48 hours, 4 weeks of adequate anticoagulation or TEE is needed before attempting cardioversion to sinus rhythm. • If TEE does not visualize the presence of left atrial thrombus, cardioversion can be performed with continuation of warfarin for four weeks after cardioversion. However, the safety of this approach has not been formally studied in atrial flutter. • Among patients with atrial fibrillation and flutter, the choice between warfarin and aspirin is based upon the estimated stroke risk using the CHADS2 score.
Ablation • Radiofrequency ablation interrupts the reentrant circuit in order to prevent the recurrence of atrial flutter. • With recurrent symptomatic Type I atrial flutter, there is a success rate of higher than 95% with ablation. • Ablation is commonly performed at the 6:00 position on the tricuspid valve isthmus. • Type II atrial flutter is also amenable to ablation and success rate is close to 95%, but recurrence is more common than Type I. • In patients with atrial flutter treated with ablation who subsequently develop a fib (56% in one study), ablation of the AV junction may need to be performed with placement of pacemaker.
Take Home Points • Typical atrial flutter (Type I) is an “isthmus-dependent” flutter involving a macroreentrant arrhythmia down a long slow path, due to an isthmus of tissue between the IVC and tricuspid annulus. • Atypical atrial flutter (Type II) is not isthmus-dependent and involves an intra-atrial reentrant circuit that is very short and related to abnormal anatomy within the right or left atrium.
Take Home Points • IV calcium channel blockers (Diltiazem or Verapamil) or beta blockers (Esmolol) may be used to control rapid ventricular rate. • The optimal outcome of atrial flutter is reversion to and maintenance of normal sinus rhythm, not ventricular rate control. • Cardioversion can be performed by electrical or chemical means. • If TEE does not visualize the presence of left atrial thrombus, cardioversion can be performed with continuation of warfarin for four weeks after cardioversion. • Radiofrequency ablation should be considered prior to starting an antiarrhythmic agent.