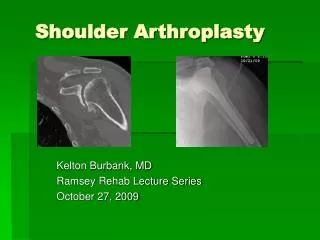
Reverse Total Shoulder Arthroplasty
Reverse Total Shoulder Arthroplasty. Reza Omid, M.D. Assistant Professor Orthopaedic Surgery Shoulder & Elbow Reconstruction Sports Medicine Keck School of Medicine of USC. Incidence of RC Tears with Osteoarthritis. 5-10%. Glenohumeral OA. Glenohumeral OA.

Reverse Total Shoulder Arthroplasty
E N D
Presentation Transcript
Reverse Total Shoulder Arthroplasty Reza Omid, M.D. Assistant Professor Orthopaedic Surgery Shoulder & Elbow Reconstruction Sports Medicine Keck School of Medicine of USC
Glenohumeral OA • Glenoid cartilage is typically spared anteriorly • Wear is more pronounced posteriorly with appearance of a “biconcave glenoid”.
Indications for RTSA • Rotator cuff dysfunction • Proximal humerus fractures • Glenoid bone loss • Revision TSA
Reverse TSA • Predictable outcome • Best TSA or Hemi is better than the best reverse • Best indication is CTA • Worst indication is revision arthroplasty • Not a good option if good FE
REVERSE TSA • Two Types: • Lateralized • Initial design of the 70’s but abandoned • Frankle design recently • Medialized • Grammont design 1991 • Most common design (zimmer, tornier, depuy, etc)
How Does A Reverse Work? • 1) Medialization/Lateralization • 2) Distalization • 3) Semiconstrained
Biomechanics • Medialization converst the shear force to a compressive force at the baseplate/glenoid interface. • Distalization tensions deltoid • Semiconstraint nature overcomes deficient cuff
Constraint • Under active conditions, a mismatch of 4mm was found to produce translations (1-2mm) that most closely reproduced those observed with the original anatomy • (Williams JOR 1996:14(6):986-993).
Benefits of Lateralization • Improved ER/IR • Improved deltoid contour • Less notching
Benefits of Medialization • Biomechanically superior (compression force at baseplate glenoid interface)
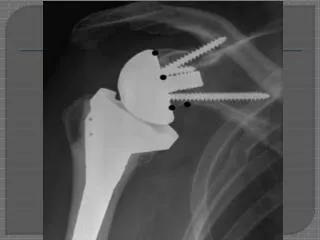
Integra Reverse Shoulder System • Central Screw • Peripheral Screws • Baseplate • Glenosphere • Humeral Insert • Humeral Body • Stem
Glenosphere • Glenospheres made of CoCr • 38mm diameter • Many options to varying patient anatomy, increase ROM and prevent scapular notching • Concentric Glenosphere, 2mm Lateralized • Concentric Glenosphere, 5mm Lateralized • 4mm Eccentric Glenosphere, 2mm Lateralized • 4mm Eccentric Glenosphere, 5mm Lateralized • 4mm Eccentric Glenosphere, Inferior Hooded 2mm Lateralized
Glenosphere Positioning • Lateralizing the C.O.R. = increased ROM, increased internal/external, decreased scapula notching. • Eccentric = ideal baseplate positioning while allowing the glenosphere to be position inferiorly and avoid scapular notching. Increases deltoid tension. • Both options together + multiple humeral body heights allow us to have only one diameter Glenosphere (38mm).
Baseplate and Screws 22mm • Glenoid baseplates made of Ti with Asymmatrix porous coating • 15mm length post (primary cases) • 25mm length post (revision and bone grafting) length options • Curved back (convex) – anatomic shape 27mm
Baseplate and Screws • Central Compression Screw • 5.5mm x (20-45mm) length in 5mm increments • Independent compression screw in various length adds for central compression of baseplate into glenoid • Peripheral polyaxial locking screws • 4.5mm x (15-55mm) length in 5mm increments • Anterior and Posterior are compression screws • Superior and Inferior are compression and then locked (Variable Angle Locking Screws)
Reverse Body • Reverse Humeral Body made of Ti with Asymmatrix porous coating • 142 degree inclination angle • Decreases scapular notching versus a 155 degree inclination • Increased glenoid access • Polished medial calcar to allow for tuberosity and soft tissue suture retention. • Asymmatrix coating allows for good secondary fixation and allows for all press fit humeral component. • Morse taper and backup screw for body to stem connection • 3 body height options • Small (30mm) • Standard (35mm) • Large (40mm)
Humeral Poly Liners & Stems • Humeral insert made of UHMWPe • Standard - +0mm, +3mm, +6mm, +9mm • Retentive - +0mm, +3mm, +6mm, +9mm • Retentive option provides more glenosphere coverage providing more stability yet increased chance for scapular notching. • Humeral Stems made from Ti for press fit applications • 11 sizes (6-16mm) 1mm increments • Humeral Stems made from CoCr for cemented applications • 5 sizes (6-14mm) 2mm increments
Humeral Preparation Stem Sizing & Trial Select Small Body Or 142 Degree Osteotomy
Humeral Preparation Humeral Reaming Reamer Body Inserter Humeral Body Trial and Inserter
Glenoid Preparation Baseplate Glenoid Wire Guide Glenosphere Glenoid Wire Guide Or
Glenoid Preparation Glenoid Reaming Baseplate Insertion Baseplate Boss Drilling
Baseplate Screw Fixation 5.5 Central Screw Preparation 4.5 Peripheral Screw Preparation and Locking Caps
Case • 60 yo RHD s/p fall