Total Hip Arthroplasty
Total Hip Arthroplasty. Contents. Hip joint anatomy What is THA Indications for THA Characteristics/Clinical presentation of indications Diagnostic Fx Radiological Fx Surgical procedures Contraindications Post op.characteristics / Clinical presentation Complications.


Total Hip Arthroplasty
E N D
Presentation Transcript
Contents • Hip joint anatomy • What is THA • Indications for THA • Characteristics/Clinical presentation of indications • Diagnostic Fx • Radiological Fx • Surgical procedures • Contraindications • Post op.characteristics/ Clinical presentation • Complications
Post op. physical therapy Ex • PhysicaltherapyMx • Principles of rehabilitation • Mx protocols of THA (APTA) • Modalities supported by research • DON'TS and DO’S • Post op. precautions • Long term followup
Hip joint • General anatomical overview
Description of THR An invasive surgical procedure that is used to remove a diseased hip joint (most commonly due to osteoarthritis) and replace it with an artificial joint or prosthesis.
Indications for THA • Disabling pain secondary to severe osteoarthritis • Inflammatory arthropathy • Avascular necrosis • Ankylosis secondary to prior infection or surgery • Trauma such as a fall – most commonly post menopausal women • Juvenile rheumatic arthritis • Benign/malignant tumors around the hip joint, and hip fractures.
complications with the internal fixation of a fracture to the femoral neck- if articular cartilage in the acetabulum is lost or when endoprosthesis have failed in acute fractures
Clinical Presentation of indications • Hip fracture: Often unable to walk, complains of vague pain in the knee, thigh, groin, back or buttock and difficulty of weight bearing. • Osteoarthritis: Crepitations are sensible or audible when the hip is moved, all the inflammatory signs. • Rheumatoid arthritis: Range of all hip movements is impaired, movement is painful, pain and stiffness when the activity is resumed after resting. Redness, joint effusion.
Dx Procedures • No specific diagnosis. • Differentiate from referred pian from the spine or pelvis. • Most helpful ways to diagnose if the patient really needs a THR - MRI, X-Ray and physical Ex specific to the particular condition.
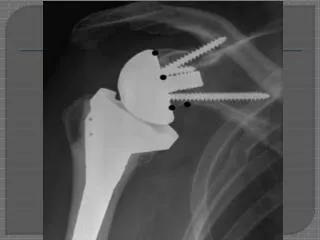
Radiological Fx Osteoporotic bones
Surgical procedures • Anterior, lateral and posterior approach. • The articulating couples (head and cup) used by surgeons are made of metal-on-polyethylene (PE), ceramic-on-PE, metal-on-metal and ceramic-on-ceramic • Important components of prosthesis are friction-coefficient, survival, stability against dislocation and fixation in bone tissue. • Osteonecrosisdue to erosion of the two components rubbing against each other
Contraindications • Active local or systemic infection.
Post op.characteristics/ Clinical presentation • Muscular atrophy and loss of muscle strength, particularly in the gluteus medius muscle and ipsilateral quadriceps • There is a major risk associated with joint instability and prosthetic loosening. • Gait dysfunction may persist for many months after joint replacement.
Physical therapy Mx • Considered according to the surgical approach and the state of the patient. • Patient desires to gain physical fitness or wishes to recover for recreational activity • Posterior approach- precautions should be taken against dislocation when exercises combining flexion, endorotation and adduction are given.
Anterior approach- combination of extension, exorotation and abduction (probability of dislocation is less great than for the posterior approach)
Principles of rehabilitation • Assessment • Reduce pain • Reduce swelling • Increases range of movement • Improve muscle strength • Aid proprioception • Mobilize patient • Prevent complications • Educate patient and family
Postoperative day 1: • Post operative assessment – subjective and objective • Check operation notes and post operative instructions • Observations - HR, BP, Drainage, Temperature • Analgesia – useful to use 0-10 scale for pain assessment • Physical observation of pain, range of movement and muscle strength • Respiration and circulation
Mx protocols of THA (*APTA) Acute phase (1-4 days) • Educate on dislocation precautions • Increase independence with function • Prevent or reduce post operative impairments.
Treatment occurs bedside, Evaluation, dangle, stand or ambulate as tolerated, Bedside exercises, THA precautions instructed (APTA) • Static contraction of the M. Quadriceps in order to have a muscular and circulatory effect. • Flexion/extension/rotation of feet and toes to prevent edema. • Education of muscular relaxation. • Upper limb exercises to stimulate the cardiac function.
Maintenance of the non-operated leg: attention should be paid to the range of motion in order to preserve controlled mobilization on the operated hip. • Bed exercise following total hip replacement is important prevent edema, improve cardiac function, etc…
Postoperative day 2: Treatment occurs bedside, Transfer training, Progress ambulation distance as tolerated with walker, Review exercises and precautions, High chair sitting and bathroom privileges. (APTA)
Postoperative day 3: Continue transfer training, Attempt gait progression to cane or crutches and stair training, Treatment session in PT gym, Progression of exercise program, Review Precautions, High chair sitting and bathroom privileges. (APTA)
Postoperative day 4: Continue transfer training, Continue gait progression and stairs, Treatment session in PT gym, Review home exercise program and ADL technique, Discharge if appropriate. (APTA)
First postoperative week: Active/passive mobilizations to gain ROM • Progressive resistance exercises • Progressive weight bearing exercises according to tolerance • Equilibrium exercises including walking with crutches/2 canes/1 cane.
Early exercises including full weight bearing exercises have shown different positive effects on the recovery of patients after THA • Amount of activity is linked to the general state of the patient.
Motion Phase (week 1-6) • This phase includes therapeutic exercise and modalities as needed. Goals of this phase include: • Muscle strengthening of the hip girdle of the operative extremity • Proprioceptive training to improve body awareness for functional training • Endurance to increase cardiovascular fitness • Gait training; discontinue assistive device approx. 4-6 weeks when there are no signs of an antalgic gait, or trendelenburg sign. • Increase ROM • Increase Strength • Return to functional activities
Therapeutic Exercises: Weeks 1-4 • AA/A/ PROM for all hip motions • Isometric quadriceps, hamstrings, and gluteal exercises • Heel slides • Balance training : weight shifting activities and closed kinetic chain activites • Gait training • Stationary bike, weeks 3-4 as advised by MD
Weeks 4-6 • Continue above exercises • Front and lateral step up and down • 4 way straight leg raise; if not contraindicated by precautions • ¼ lunge • Sit to stand exercises • Pushing and pulling exercises • Aquatic program
Criteria for progression: • AROM 0-110 degrees • Voluntary quadriceps control • Independent ambulation of 800ft without an assistive device, antalgia, or deviations • Minimal complaints of pain and inflammation
Intermediate Phase (week 7-12) Goals for this phase include: • Good Strength for all lower extremity musculature • Return to most functional activity and participation in light recreational activities • Progress exercises in Movement phase by adding resistance and repititions. • Assess lower extremity and trunk stability, provide open and closed chain exercises as necessary to fit the needs of the individual patient
Initiate endurance program ( pool or walking) • Initiate age appropriate balance and proprioception training Criteria for progression: • 4+/5 MMT on all lower extremity musculature • Minimal to no complaint of pain and swelling
Advanced strengthening and higher level function stage (week 12-16) Goals for this phase include: • Return fully to appropriate recreational activities • Enhance strength, endurance, and proprioception Therapeutic Exercises: • Continue to progress previous exercises • Increase duration of endurance activities • Carrying, pushing, pulling activities • Return to specific recreational activities ( golf, tennis, walking, biking) • Return to work tasks
Criteria for progression: • Non-antalgic independent gait • Independent step over step stair climbing • Pain free AROM • 4+/5 MMT on all lower extremities • Independent with home exercise program • Age appropriate balance and proprioception
Modalities supported by research • Cryotherapy • Thermotherapy • Electrical stimulation
Long term follow up • wear is not a short term problem • Overweight and overuse are favorable factors for polyethylene wear, or breakage. • loosening is not a short term problem • Overweight and trauma are favorable factors for bone loosening
Tell your doctor or dentist that you have a prosthetic device so that in case of infection he gives you adaquatetreament with antibiotics to prevent an infection of the prosthetic joint. • Do exercises at home. Sports activities are possible • According to comorbidity, age, range of motion and stability ; waiting 3 to 6 months after a THA is a current recommended waiting time for return to sporting