Download
1 / 32
330 likes | 764 Vues
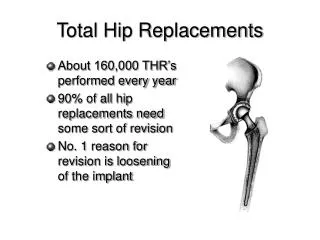
Total Hip Arthroplasty after Hip Fusion. Wayne Paprosky M.D. , F.A.C.S. Indications for Conversion. Fibrous Ankylosis non-union Solid Fusion. Pre-op Xrays. RO. F. Pre-op Xrays. H. G. Indications for Conversion. Painful pseudarthrosis requiring THA 29.6 % - 57.6%

E N D
Total Hip Arthroplasty after Hip Fusion Wayne Paprosky M.D. , F.A.C.S.
Indications for Conversion • Fibrous Ankylosis non-union • Solid Fusion
Pre-op Xrays RO F
Pre-op Xrays H G
Indications for Conversion • Painful pseudarthrosis requiring THA • 29.6 % - 57.6% • Pain in affected hip after attempted fusion • C.T. scan • Fluoroscopic exam
Solid Arthrodesis – Hip Painfull • Pain in other joints • Functional disability • i.e. sitting or driving • Excessive pelvic rotation • Increased motion of other hip • Increased flexion of ipsilateral knee • Increased abduction – adduction movements of both knees
Arthrodesis • Knees & contralateral Hip can develop DJD
Arthrodesis • Most common reasons Fusion -> T.H.A. • Low back pain – 56.5% - 75.6 % • Multilevel DJD of L.S. spine at 30 yrs: post arthrodesis • Malpositioning of fused hips in excessive abduction main reason for low back pain
Arthrodesis • Contralateral hip pain with DJD -> THA • 36 % (Callaghan) • Because R.O.M. increases and extra support required of hip • Relative abduction secondary to fusion = increased joint reactive force
Arthrodesis • Loss of function from immobility or malposition of fused hip, second most common reason for THA
Arthrodesis • Results of conversion • Relief of low back pain 73% – 93% • Correction of L.L.D. • Improved sitting • Improved mobility
Arthrodesis • Abductor function • Less predictable 2-5 yrs post-op • Always will have some weakness • 78% need 1 or 2 crutches • 87% positive Trendelenberg • Residual weakness • Major dissatisfaction (Harding)
Arthrodesis • Do not convert only for immobility in the absence of significant pain
Arthrodesis • Abductor function better after THA • Better if fusion occurred as adults • Abductor fully developed
Arthrodesis • Knee pain unimproved in 33% of conversions
Results • Clinical and Radiographic results • Harding • 112 patients • 1% stems loose at 8 yrs (cemented) • Kilgus • M.F.R. 7.9 % at 7 yrs. (cemented) • No cementless series available
Results • Complications • Infections • 1.9 % - 15.3% • Dislocation • 1.7% - 6.5% (Harding) • Nerve Palsy • 1.8% - 13.4 % (Sciatic, Peroneal) • Amstutz. 3.6% (Femoral nerve)
Key step: Separation of femur from pelvis without damage to pelvis or femur
Suggestion: • Use Gigli saw • safe separation • leaves abductors intact
Trochanteric Osteotomy or Slide Addresses Proximal deformity only
Surgical Technique • ETO to remove deep overgrown femoral hardware • Do not strip abductors • Identify and protect sciatic nerve
Extended Trochanteric Osteotomy in Complex Primary T.H.A. Craig J. Della Valle M.D., Wayne Paprosky M.D., F.A.C.S. et. al., J.B.J.S. AM 2003, 2385-2389
MB 7 yrs MB
Conclusion • Do not resect neck to high • Avoid pelvic violation • Avoid fracture of ischium and pubis • Use guide wires & xrays if necessary • Meticulously expose acetabulum • Iliopsoas release usually necessary
Conclusion • Proximal femoral anatomy distorted • Special implants (ie.CDH) • May need sub troch osteotomy • Bypass removed hardware stress risers • Do not over lengthen leg
Conclusion • Beware of absent abductors from previous arthrodesis surgery • May need constrained liner • Immobilize for 6 weeks in abduction brace