Download
1 / 32
320 likes | 557 Vues
HKCEM College Tutorial. A man with Dyspnea . Author Dr Lau chui ling/Dr Lee Fu Tat July 2013. Chief Complaint. Chinese M/60 Brought in by ambulance Severe SOB LOC 5 min at home. Triage . Deep Dyspnoea Full consciousness BP 80/56mmhg, p 120/min; RR 36/min, T36.8 ℃

E N D
HKCEM College Tutorial A man with Dyspnea Author Dr Lau chuiling/Dr Lee Fu Tat July 2013
Chief Complaint • Chinese • M/60 • Brought in by ambulance • Severe SOB • LOC 5 min at home
Triage • Deep Dyspnoea • Full consciousness • BP 80/56mmhg, p 120/min; • RR 36/min, • T36.8℃ • SpO2 92 % with high flow oxygen mask • What triage category would be appropriate ? Triage category II
What would be your initial Management? • Airway–patent • Breathing–Tachypnoea,RR36/min, pleural rub. • Circulation • Elevated venous pressure • Pulse 120/min, • BP80/56mmhg • D -alert Oxygen Cardiac Monitor ECG BP/P SpO2 IV access IVF
Past History • History of CA colon • Right hemicolectomyand chemotherapy • FU PMH oncology • NKDA • Trial on TCM for 2/12 • No history of asthma
What are your differential diagnosis? • GI bleeding with hypovolaemic shock and anaemia • Lung metastasis +/- Pleural effusion • Chest Infection • Septicemia shock due to neutropenia • Pericardial effusion with tamponade due to metastasis • Arrhythmia due to herbal medicine • Acute renal failure with metabolic acidosis due to toxic effect of herbal medicine • Acute Pulmonary Embolism • Others
Physical Examination • CVS: • JVP rise, Neck vein distended • BP 80/50mmhg, pulse 120/min • S3 gallop • Abd: • - old laparotomy scar, • - hepatomegaly, • - non tender • Left calf swelling than right, • both ankle edema • GC: - alert - Pallor &cyanotic - sweating • Resp: - distress - RR40/min, - Use of accessory muscles - Trachea central - Air entry equal, no added sound
What is the most likely diagnosis in this patient&Why ? DVT with Acute Pulmonary Embolism
What are the Clinical Probability Assessment of PE ? 1. Well’s Risk Score (level 2 evidence) http://emedsa.org.au/EDHandbook/medicine/Respiratory/PE/PEScores.htm 2. Geneva score (level 2 evidence) http://www.medicalapps.ch/Geneva_Score.aspx (On line calculator) 3. Pisa model (level 1 evidence) http://www.ifc.cnr.it/pisamodel/pisamodel2/calcolo2.html(Onine calculator without CXR) http://www.ifc.cnr.it/pisamodel/pisamodel1/calcolo.html (Online calculator with CXR) 4. Charlotte rule http://www.nbgh-er.com/Simplified_criteria_for_PE.pdf
What would you do if the clinical probability is low or moderate? • D-dimer (detect fibrin) • Sensitive 98-100% ,non-specific • NPV 90-100%, • < 500 ug/l (500ng/ml)(ELISA) reliably rule out PE • No further test is required
What would you do if low probability Patients with abnormal D dimer • Contrast enhanced MDCTA (multi detector –row computed tomography angiography) Level 1 • Venous USG of Lower Limbs for DVT or CT venography of leg veins • Computed tomography (CT) angiography • VQ scan is useful in probability assessment and less radiation exposure in comparing with CT angiography but is not easily available in Hong Kong • Pulmonary angiogram (gold standard) but is usually not available • Filling defect or sharp cutoff of affected artery • Non occlusive emboli have a Tram-track appearance. • Spiral CT (not for peripheral embolism)
What would you do ifHigh Clinical Probability of PE ? • D dimer is not helpful because of low negative predictive value • D dimer is also not helpful in patients: • older than 80 years of age • Hospitalized • Have cancer • Pregnant woman D dimer are frequently elevated in such patients The New England Journal of Medicine 359.26 (Dec 25, 2008): 2804-2813.
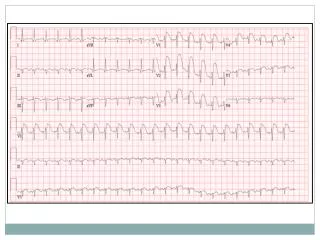
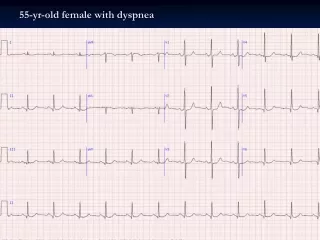
only 20% of patients with proven PE have ECG abnormalities Sinus tachycardia (Commonest) RBBB, RAD T inversion in III & aVF or V1-V4 S1Q3T3 (10-50%) Not Sensitive Not specific http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2735159/ What are the ECG features of PE ?
What are the radiological features you would look for in patient with acute PE ? Most CXR are normal (25%) NOT SENSITIVE NOT SPECIFIC
Picture from NEJM. Sokoloveand Offerman 345 (18): 1311, Figure 1 November 1, 2001 C B A • A: Hampton's hump - peripheral wedge of airspace opacity at the left lung base and implies lung infarction • B: A ventilation–perfusion scan showed normal ventilation images and loss of perfusion to the entire right • upper lobe as well as to the anterior, lateral, and medial basal segments of the left lower lobe (Panel B). • C: Westermark's sign: regional oligaemiain the right upper lung field.
Other CXR features • Knuckle sign : Abrupt tapering /termination of pulmonary vessel) • Fleischersign : prominent pulmonary artery (20%) • Palla'ssign : enlarged right descending pulmonary artery • Atelectasis/infiltration • small pleural effusion (35%) • elevated hemidiaphragm • After 24-72 hours, 1/3 PE develop focal infiltrates indistinguishable from an infectious pneumonia http://radiopaedia.org/articles/pulmonary_embolism
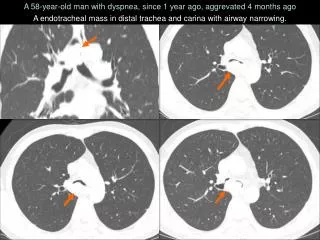
What are the abnormalities CT Thorax & Abdomen of our patient? Multiple liver metastases Extensive pulmonary embolism noted laterally, involving distal right and left pulmonary arteries and extending into smaller branches distally
Progress • Patient become increasingly drowsy and dyspnea • Vital signs: • BP 60/- pulse 150/min ,thready • RR 40/min • SpO2 difficult to get due to poor perfusion Is the Pulmonary Embolism Massive or Submassive PE? Why?
What is Massive PE? Definition: • Sustained hypotension SBP < 90mmHg Drop in SBP of at least 40 mmHg for at least 15 minutes or requiring inotropic support. Not due to a cause other than PE, such as arrhythmia,hypovolemia, sepsis, or left ventricular dysfunction • Persistent profound bradycardia (heart rate <40 bpm with signs or symptoms of shock) • Pulselessness • Early Mortality at least 15% • The degree of haemodynamic compromise is the most powerful predictor of in-hospital death http://circ.ahajournals.org/content/112/2/e28.full What other investigations will you do now?
Echocardiogram Look for signs of acute pulmonary hypertension and right ventricular overload Sensitivity 100% for massive PE if there is RV enlargement or dysfunction Valuable alternative if CT is not immediately available or if the patient’s condition is too unstable for transfer to CT suite
Transthoracic Echo cardiogram features in Massive Pulmonary embolus • Dilated RV, hypokinestic RV, Tricuspid regurgitation, IVC dilated but not collapse • Mc Connell’s sign: Normal RV apex contractility with akinesia of RV free wall • LV small and hyperkinetic • Paradoxical interventricularseptal motion in those with high RV pressure • Thrombus occasionally seen in right heart chambers, RV thrombus. • Pulmonary regurgitation and severe acute pulmonary hypertension(Doppler) http://www.youtube.com/watch?v=qJvVbEe2yoc
USG of Lower Limb • What Mode? • What will be your finding?
USG features of DVT • B mode Presence of clot would prevent the collapse of the vein when being pressed by the probe • Doppler Valsalvamaneuver & respiration- affect the pattern of wave forms of spectral doppler. Loss of this effect means presence of obstruction between the diaphragm & the study venous segment • Augmentation Gently compress the region distal to the probe would increase the flow through the study venous segment. Loss of such effect means presence of obstruction between the site of compression and the study segment http://www.youtube.com/watch?v=Jg0TwINcZqE
What is your management? • Supportive & Specific treatment • ICU care Supportive Treatment • 100% O2 • Fluid bolus NS 500 ml IVI • Inotrope Dopamine or Dobutamine or Adrenaline What are your specific treatment?
Empirical anticoagulation therapy • Immediate full anticoagulation is mandatory for all patient suspected of having DVT or Pulmonary embolism. • All patients should have baseline coagulation studies • Diagnostic investigations should not delay empirical anticoagulant therapy
Haemodynamically Stable • Subcutaneous low molecular weight heparin(LMWH) (ACCP 1A) • Enoxaparin1mg/kg SC Q12h, Tinzaparin(A/V in HA) andDalteparin • At least as effective as UFH • Reduced mortality and less risk for major bleeding than UFH • Cost Savings • More predictable pharmacokinetics than UFH • With cancer LMWH for first 3-6 months (ACCP grade 1A) • IVUnfractionHeparin 80 unit/kg bolus then 18 unit/kg/h x 6 hrs(ACCP grade 1A) • Need to monitor APTT (1.5 to 2.5 times of control) frequently • Potential heparin-induced toxicity, especially heparin induced thrombocytopenia • Pentasaccharides (not A/V in HA) • Fondaparinux5-10mg daily • At least as effective as Enoxaparin
Our case Management in the ward • Clexane (Enoxaparin) • Warfarin • Keep INR:2-3 • Take over to palliative uniton Day 5 after ICU care • No more dyspnea and BP/P stable and started mobilization What other drug or treatment you would like to consider if hemodynamic compromise ?
Haemodynamically Unstable • Fibrinolytic therapy / Thrombolytic therapy (ACCP grade 1B) • Indicated for massive or haemodynemic unstable pulmonary embolism (PE) . • Improvement of hypotension in response to hydration or pressors does not remove the indication for immediate fibrinolysis. • Hypotension occurred is a sufficient indication that the patient has exhausted cardiopulmonary reserves at high risk for sudden collapse and death. • Evidence indicates that the mortality rate can be cut in half by early fibrinolysis. • Interventional radiology has made it possible to perform transcatheter fibrinolysis for patients who have DVT without evidence of PE.
Fibrinolyticthearpy FDA approval • Streptokinase250,000 U over 30 minutes followed by 100,000U/h for 12- 24 h • Streptokinase 1.5 megaU over 2 h is as effective as rt-PA • rt-PA (Alteplase) 100 mg over 2h • Urokinase FDA not approval • Reteplase: more effective in large or old clots • Tenecteplase (TNK) http://emj.bmj.com/content/22/11/766.full
Unstable BP <100mmhg and C/I to fibrinolytic therapy Surgical Care: (interventional catheterization techniques) • Catheter fragmentation extraction/Surgical thrombectomy/Percutaneous catheter embolectomy • Right atrial and left atrial or veno-atrial bypass. • Vena cava filter • Anticoagulation contraindicated • Recurrent PE despite anticoagulation