Download
1 / 29
290 likes | 463 Vues
A 35-Year-Old Man with Dyspnea. Cardiology Case DISCUSSION VICTOR TSENG, md Andrew Mccue , m4 November 22, 2013. Chief Complaint/HPI. 35 YEAR OLD MAN COUGH, CORYZA, FEVER started 9/5/2013 minimal pinkish sputum, slowly progressive, mild wheeze, no chest pain

E N D
A 35-Year-Old Man with Dyspnea Cardiology Case DISCUSSION VICTOR TSENG, md Andrew Mccue, m4 November 22, 2013
Chief Complaint/HPI 35 YEAR OLD MAN COUGH, CORYZA, FEVER • started 9/5/2013 • minimal pinkish sputum, slowly progressive, mild wheeze, no chest pain • home T 39◦C with occasional rigors • ROS: (-) pharyngitis, (-) adenopathy, (-) reflux, (-) sinus congestion, (+) rhinoconjunctivitis, (+) malaise, (+) myalgias DYSPNEA • became noticeable on 10/15/2013 • new 4-pillow orthopnea, + PND, slight pedal edema to thighs, now chairbound with SOB • ROS: (-) palpitations, (-) pleurisy, (-) presyncope, (-) unilateral calf swelling
MEDICAL HISTORY • Ph+ ALL (August 2012) s/p URD PB SCT (May 2013) • good engraftment • molecular remission • Grade 2 GVHD Colitis and Dermatitis • E. faecalisbacteremia and severe sepsis (Feb 2013)
SOCIAL HISTORY • Born in India, immigrated to U.S in 2010 • Software engineer for Coca Cola™ • Never smoker, never EtOH, no recreational/illicit drug use • No environmental allergies • Never homeless, incarcerated, communal habitation • Married and monogamous • Has 5 y/o son who was recently ill with upper-respiratory symptoms
MEDICATIONS • acyclovir 400 mg, PO, q12hr • albuterol 90 mcg/inh MDI QID, PRN • benzonatate 100 mg, PO, TID, PRN • dasatinib 40 mg, PO, qDay • lorazepam 0.5 mg, PO, q6hr, PRN • oxycodone 10 mg, PO, q4hr, PRN • pentamidine Inhale, qMonth
PHYSICAL EXAM • GEN: diaphoretic, severe distress • HEENT: sclera with suffusion, posterior pharynx with erythema, oral mucosa moist, no thyromegaly or bruit, no sinus tenderness • NEURO: AO x 4, normal sensorium, no lateralizing motor or sensory deficits • COR: very rapid regular, summation gallop, no rubs, nondisplaced apical impulse • VASCULAR: • v: engorged IJV,+ HJR, + Kussmaul’s • a: pulsus pressure = 20, pulsus alternans (2+/1+), warm extremities • RESPIRATORY: speaking in clipped sentences, clear lung fields, good air entry • ABDOMEN: soft, flat, non-tender, non-distended, • MSK: normal ROM, no joint effusions • SKIN: no rashes • LYMPH: no cervical adenopathy
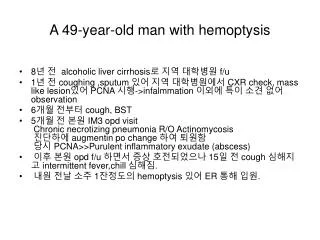
LABORATORY DATA (PART 1) 5.6 2.9 9.4 17 135 100 13.5 0.9 2.0 16.0 161 164 40.5 4.3 0.7 25 438 172 104 Tn-I/CK-MB Pending
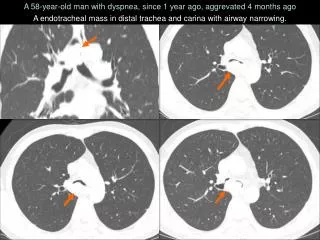
CORONARY ANGIOGRAPHY (LHC) LAO Right System RAO Left System
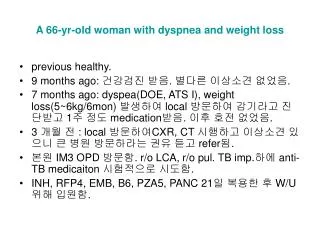
HEMODYNAMICS Art SpO2 = 99% PA SpO2 = 58% 20/11 (25/5) CO (Fick) = 3.4 LPM 18 (≤8) 11 (≤12)
SIDE NOTE CO = HR×SV “Sometimes, the scariest rhythm in the CCU is bad sinus tacycardia” Robert Cole, MD HF/CCU Attending
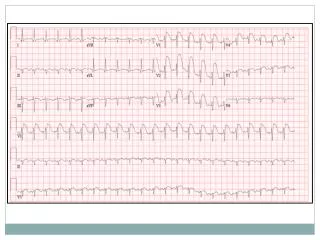
DIAGNOSIS DIAGNOSIS • Fulminant Lymphocytic Myocarditis • RSV Bronchiolitis COMPLICATIONS • Cardiogenic Shock • Acute RV Failure • Ventricular Tachycardia Storm
HOSPITAL COURSE • Transferred to CCU • Swan-Ganz (PA) Catheter for tailored IVF and inotrope therapy • High-dose IV Steroids x 3d then PO taper • ST elevations resolved by day 4, Tn-I peaked at 34.7 ng/mL • Shock/Tachycardia resolved by 1 week • Ribavirin + Palivizumab (Synagis™), aggressive pulmonary toilet • LifeVest for protection of VT • RVEF with recovery to normal by 2 weeks • Good rehabilitation and discharged home • Doing well
MYOCARDITIS FRANK CORRIGAN III, MD
Inflammatory Cardiomyopathy • Myocarditis w/ Myocardial Dysfunction • Most Common Etiologies: Parvo B19, HHV 6 • Findings predictive of subsequent death or transplantation • Syncope (RR 8.5), bundle branch block (RR 2.9), LVEF <40% (RR 2.9) • Secondary pHTN (mean PAP) most predictive of death. • Each 5mmHg increase from baseline MPAP, mortality increased with Hazard Ratio 1.85 (HR 1.23 in those without myocarditis)
Classification • Giant Cell • etiology unknown. Most severe symptoms. Mediated by T cells and giant cells • Fulminant • Most commonly a viral etiology • p/w with acute HF up to 2 weeks after distinct viral prodrome. • Acute • p/w less distinct symptom onset. Have established ventricular systolic dysfunction.
Outcomes • Patients with fulminant myocarditis, although more severely ill, are more likely to recover than those with acute myocarditis. • At 11 year follow-up, transplant-free survival was 93% fulminant vs. 45% acute. • Giant Cell Myocarditis: rate of death or cardiac transplant 89%. Median survival from symptom onset 5.5 months
Who to Biopsy? • New onset HF of ≤ 2 weeks duration associated with a normal LV chamber size and hemodynamic compromise • New onset HF of 2 weeks – 3 months duration associated with a dilated LV • New ventricular arrhythmias • 2nd or 3rd degree AV block • Failure to respond to usual care within 1-2 weeks
EMB vs. Cardiac MR • CMR shows most common site of focal involvement was epicardial surface of LV free wall. • Study showed EMB + myocarditis in 19/21 patients directed by CMR imaging (suggestive of myocarditis) *Most EMBs obtained from RV side of IVS
Dallas Criteria • Active myocarditis- an inflammatory infiltrate of the myocardium with necrosis &/or degeneration of adjacent myocytes not typical of ischemic damage associated with CAD • Borderline myocarditis- the inflammatory infiltrate is too sparse or myocyte injury is not demonstated
References • Cooper, LT Jr. 2009. Myocarditis. NEJM 360(15):1526 • Goldberg, LR, Suk, J, et at. 1999. Predictors of adverse outcome of biopsy-proven myocarditis. J Am Coll Cardiology. 33:A850. • McCarthy RE, Boehmer JP, et al. 2000. Long-term outcome of fulminant myocarditis as compared to acute. NEJM 342(10):690 • Mahgholdt H, Goedecke C, et al. 2004. Cardiovascular magnetic resonance assessment of human myocarditis. Circulation. 109(10):1250. • Aretz HT, Billingham ME, et al. 1987. Myocarditis: a histopathologic definition and classification. Am J Cardiovasc Pathol. 1(1):3.