Download
1 / 33
330 likes | 639 Vues
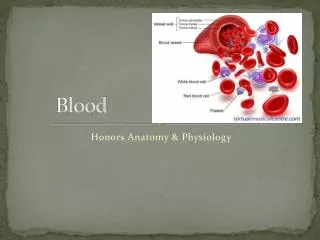
Blood. Chapter 17. Blood Composition. Formed Elements = cells (~45%) Red Blood Cells (RBCs, Erythrocytes) White Blood Cells (WBCs, Leukocytes) Platelets Plasma = soluble materials (~55%). Blood Composition. Percentage of blood that is formed elements – hematocrit Normal Values

E N D
Blood Chapter 17
Blood Composition • Formed Elements = cells (~45%) • Red Blood Cells (RBCs, Erythrocytes) • White Blood Cells (WBCs, Leukocytes) • Platelets • Plasma = soluble materials (~55%)
Blood Composition • Percentage of blood that is formed elements – hematocrit • Normal Values Male 42-52% Female 37-47% • Note: WBCs take up <1%, Plasma is majority (55%)
..Blood Composition • Total Blood Volume Male = 5-6 L Female = 4-5 L
Plasma • Straw-coloured fluid • ~91-93% water, 7% proteins, 1.5 % other solutes • Nutrients • fats, carbohydrates (glucose), amino acids, minerals, vitamins • Wastes – by-products of living tissue metabolism (creatinine, lactic acid, ammonia, CO2, etc.)
Plasma • Plasma Proteins • Albumin (54%) - osmosis and carriers • Globulins (38%)- antibodies • Fibrinogen (7%)- clotting • Other: • oxygen • Electrolytes (Na, K, Ca, Cl, HCO3) • hormones
Plasma Proteins • Functions: • Osmotic • albumins pull water back into capillary by osmotic pressure • Antibodies • globulins act to recognize foreign material • Buffers • limit pH changes by taking up H+ • normal pH of blood: 7.35-7.45 (slightly alkaline) • Lipid Transport • Lipoproteins are complexes of fat and protein • eg. LDL’s and HDL’s (High/Low Density Lipoproteins
RBCs • Biconcave discs, anucleate, essentially no organelles • Sickle cell – see next slide • 5 million cells/mm3 • Normal Values Male 4.5-6.5 x 1012 /L Female 4.2-5.5 x 1012 /L • Why do men have more? • Does this match with hematocrit values?
Sickle Cell Anemia • Inherited condition – predominantly African gene pool • cells lose the biconcave shape when in low oxygen (exercise may deplete O2) • becomes sickle shaped – get lodged in capillaries (often in lungs) – painful and infections can start • Survived genetic selection in Africa because SCA patients don’t tend to suffer as badly from malaria
RBCs • ~ 10,000 new cells are made every second to replace 10,000 cells that have died in that second • Where do they get produced? • red bone marrow • Where are they destroyed? • the spleen – recovers iron in heme, uses globin to make amino acids • recycling at its finest
RBCs • Cells have no nuclei • packed full of hemoglobin – almost 1/3 of the volume • Normal Values Male 16 2 g/100 mL Female 14 2 g/100 mL • note: g/100 mL is sometimes said “gram percent”
RBCs • All that hemoglobin (abbrev. Hb) is meant to carry oxygen • Hypoxia – tissue is starved of O2 – • if Hb does not have enough oxygen, then hypoxia • lips and other tissues may appear blue = cyanotic • When Hb combines with 4 molecules of O2, it’s called Oxyhemoglobin • Loads in lungs • most oxygen in blood is carried this way with some in plasma • most carbon dioxide is carried dissolved in plasma with some in Hb. • What is Deoxyhemoglobin? Where is it formed? • What is Carbaminohemoglobin? Where is it formed?
WBCs • Formally called Leukocytes • nucleated • 8,000/mm3 (4 to 10 x 109 /L) • (yes, that’s 4 to 10 billion per litre) • if values fall below this – leukopenia (low WBC count) • if values are above this – leukocytosis (high WBC count) • Why would either occur?
WBCs • To Major Groups of Leukocytes • Granular • granules clearly appear within the cytoplasm • form ~70% of all leukoctyes • Agranular – no such granules • Wright’s stain – two dyes produce a neutral stain • Eosin (red) – acidic dye • Methylene blue – basic dye
Granular WBCs • Neutrophils – 60% of total (most common) • pale lilac in stain (granules take up both red and blue dyes – neutral) • nucleus often multi-lobed • Phagocytic – bacteria slayers • ameboid movement in tissues • get in tissues by diapedesis = “leaping across” – move across capillary membranes into tissues • accumulate as pus around wounds
Granular WBCs • Eosinophils – 3% of total • deep red nucleus and lighter red granules attract red dye (eosin) • nucleus looks like phone receiver (bilobed) • Increase in response to • parasitic worms – tapeworms, flukes, pinworms, hookworms) • allergies – may lessen response
Granular WBCs • Basophils – 1% of total (rarest of all) • granules stain purplish-black – the basic (methylene blue) dyes • nucleus U or S shaped, with obvious constrictions • granules contain the Chemicals • Histamine – inflammatory response, promotes leaky capillaries (edema), dilates blood vessels and attracts neutrophils • Heparin – anticoagulant • Function is very similar to Mast cells, though unrelated
Agranular WBCs • Monocytes – 3-8% of total • largest of all leukocytes (several times an RBC) • nucleus U or kidney shaped, with obvious constrictions • become macrophages • migrate to alveoli in lung, connective tissue beneath skin, liver (fixed in place – called Kupffer cells), lymph nodes • destroy bacteria cells and viruses by phagocytosis – even some cancer cells • did you know…. • a Kupffer cell can destroy a bacterium in < 1/100 seconds?
Agranular WBCs • Lymphocytes – 25-33% of total (2nd most common) • nucleus stains dark-purple, fills most of cell • most often found in lymph nodes, spleen • important in immune response to disease • T cells • mature in the Thymus gland • act against virus-infected cells and tumour cells • B cells • mature in bone marrow • produce antibodies to recognize foreign material • Lymphoblasts • produce new lymphocytes and monocytes • so, did you notice the three platelets?
Platelets • Thrombocytes (Platelets) • megakaryocyte fragments = platelets “large nucleus cells” cell fragments • (not really cells at all) – only ¼ size of lymphocytes • only 400,00/mm3 (140-440 x 109/L) • Note: serum is plasma without platelets won’t clot
Hemostasis • Hemostasis = “blood halting” • the formation of a blood clot • loss of blood is stopped when vessels rupture – usually takes only 3-6 minutes • Overview: 3 stages • vascular spasm • dramatic vasoconstriction slow blood flow reduce losses • platelet plug formation - platelets ‘stick’ (adhere) to the wound (collagen fibres) and each other, creating a plug • platelets enhance vascular spasm - serotonin • platelets attract other platelets - ADP • coagulation • cascade of reactions blood transforms into a gel • results are due to a fibrinogen mesh that traps blood cells and seals the hole
Hemostasis • Platelets don’t stick to normal (undamaged) endothelium (lining of b.v.’s) or to each other – why? • negative charge of healthy tissue repels them (platelets are also negatively charged) • Damaged tissue loses its negative charge platelets adhere to wounds in b.v. (exposed collagen fibres) • the Platelet Plug is formed, reducing loss of blood
Hemostasis • Plasmin • as the wound heals, clot is dissolved • plasmin does this – starts within 2 days of clot formation • dissolves fibrin of clot • Purpura • small reddish or purple spots on skin - petechiae • sub-q bleeding from small vessels • results from insufficient platelet count (thrombocytopenia) • Serotonin • released by platelets • enhances vasoconstriction reduces blood loss
Clotting • Two pathways of clot formation • Intrinsic – “found within” • Blood can clot on it’s own in a tube with no external stimulus • Extrinsic – “found without” • Blood clots in response to stimuli from outside eg. chemicals released from damaged cells/tissues • shorter (quicker) path bypasses many steps of intrinsic path • Notes: • There are over 30 substances involved • Many (the “Factors”) are numbered I to XIII • the numbering is NOT in the sequence in which the reaction proceeds • Calcium is ABSOLUTELY essential for clot formation • the main difference between extrinsic and intrinsic pathways is: • extrinsic is a shorter path because of the use of Tissue thromboplastin • all other steps past that stage are shared in common
Clotting • Extrinsic Pathway to a Clot • fastest of the two pathways (shortcut) • Tissue Thromboplastin “thrombo” = clot “plastic” = to form • aka Tissue Factor (TF) - produced by damaged cells • becomes Factor X (needs Ca2+) • Factor X • which becomes Prothrombin activator (needs Ca2+) • Prothrombin activator • converts Prothrombin (plasma protein) into Thrombin (enzyme) (needs Ca2+)
Clotting • Extrinsic Pathway to a Clot (cont’d.) • Thrombin causes fibrinogen (plasma protein - soluble) to polymerize (join together) into long fibrin strands (insoluble) • Thrombin also activates factor XIII • factor XIII + Ca2+ causes fibrin strands to cross-link forming a web or mesh • Fibrin mesh traps formed elements (platelets, blood cells and fibres) in blood • creates a clot that seals the wound over 3-6 minutes after injury
Clotting • Intrinsic Pathway to a Clot • longer pathway • provoked by • plaques that become rough • lining damaged by inflammation • rupture of minor vessels • platelets adhere to collagen fibres exposed and to themselves • Hageman Factor (Factor XII) • becomes activated by collagen fibres (needs Ca2+) • a cascade through four (4) Factors (needs Ca2+)to become • Factor X • which becomes Prothrombin activator (needs Ca2+) • The rest is the same as for the extrinsic pathway …
Helpers along the way • Vitamin K • used indirectly – required by liver to make many of the clotting Factors • Plasma proteins • fibrinogen is converted to fibrin • prothrombin is converted to thrombin • plasmin will dissolve clots • Anticoagulant • prevents clotting eg. heparin (from basophils and mast cells)
More on Clottin • Thrombosis • formation of a clot • causes include • injury to b.v. • congestion (slow blood flow) • polycythemia (viscous blood due to RBC’s • hypercoagulability – smoking or high fat diet promotes platelet adherence • Embolis • a mobile clot
What can you do? • To hasten the formation of a clot • apply gauze (surface for platelets to adhere) • apply heat • sutures • apply fibrin • apply thrombin