SPINAL STENOSIS
580 likes | 962 Vues
SPINAL STENOSIS. Jung U. Yoo, M.D. Professor and Chairman Department of Orthopedics and Rehabiliatation Oregon Health and Science University. STABILITY. ORDINARY ACTIVITIES MAY GENERATE OVER 1000LB OF FORCE. MOTION. NEUROPROTECTION. SPINAL CORD NERVE ROOTS. PATHOPHYSIOLOGY.

SPINAL STENOSIS
E N D
Presentation Transcript
SPINAL STENOSIS Jung U. Yoo, M.D. Professor and Chairman Department of Orthopedics and Rehabiliatation Oregon Health and Science University
STABILITY • ORDINARY ACTIVITIES MAY GENERATE OVER 1000LB OF FORCE
NEUROPROTECTION • SPINAL CORD • NERVE ROOTS
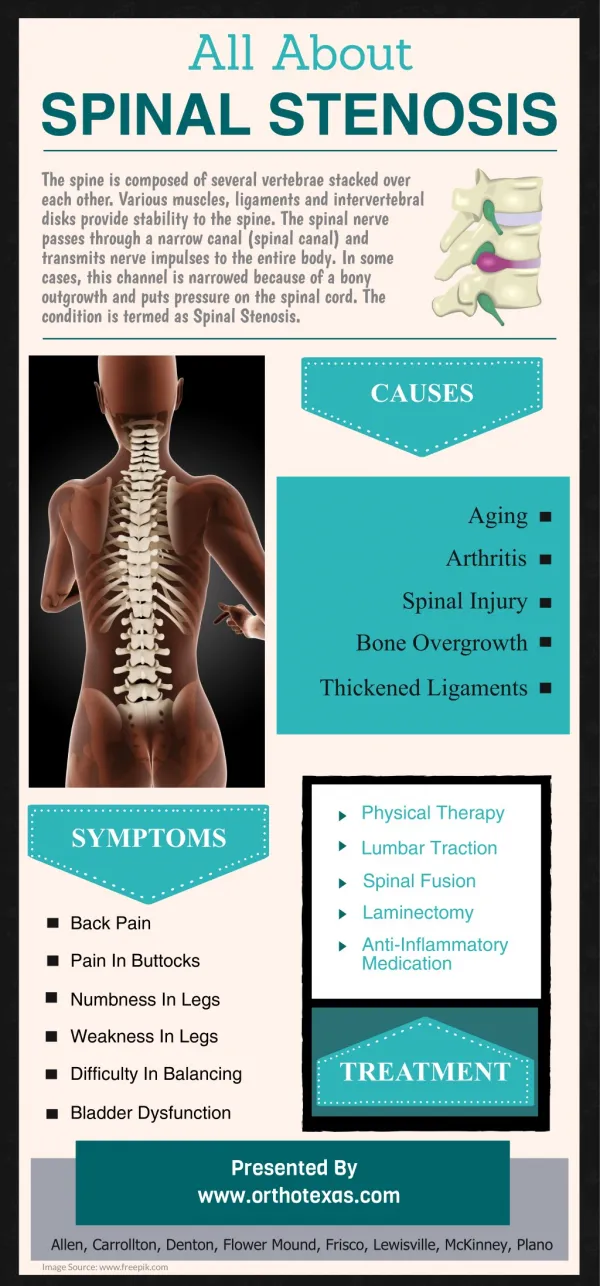
PATHOPHYSIOLOGY • “Three-joint Complex” • a large tripod with the disc as the front support and two facet joints as the back supports • Any alteration in one of these joints can lead to damage to the others
FORAMINAL STENOSIS • Compresses the exiting nerve root
CANAL SHAPE • Round • Triangular • Trefoiled (15%) • Trefoiled & asymmetric
PREVALENCE • Most common indication for spinal surgery in patients over 60 y.o. • 400,000 Americans are estimated to have spinal stenosis
STENOSIS • Narrowing of the spinal canal or neuroforamina • causing a symptomatic compression of the neural element.
SYMPTOMS • Neurogenic claudication • Radicular pain • Weakness • Sensory abnormalities • Back pain
PHYSICAL FINDINGS Physical Finding Literature Review • Limited lumbar extension 66-100% • Muscle weakness 18-52% • Sensory deficit 32-58% • Katz JN, et al: Diagnosis of lumbar spinal stenosis. Rheum. Dis. Clin. North Am. 20:471-483, 1994
NEUROGENIC CLAUDICATION • Cardinal symptom of lumbar stenosis • Progressive pain and/or paresthesia in the back, buttock, thigh and calves brought on by walking or standing, and relieved by sitting or lying down with hip flexion
DIFFERENTIAL DIAGNOSIS • Vascular claudication • Osteoarthritis of hip or knee • Lumbar disc protrusion • Intraspinal tumor • Unrecognized neurologic disease • Peripheral neuropathy
FORAMINAL STENOSIS • Root symptoms • Unilateral • No claudication • Acute or chronic
LATERAL RECESS STENOSIS • Claudication • Radicular pain • Weakness is rare • Acute or chronic
CENTRAL STENOSIS • Varied presentation • Classically with neurogenic claudication • Some may only have back pain • Rarely painless progressive weakness
X-RAY • Screening exam • Stenosis cannot be diagnosed
X-RAY • Instability such as scoliosis or listhesis
CT SCAN • Difficult to diagnose stenosis • Replaced by MRI • May be useful for those who cannot have an MRI
CT SCAN • Excellent bony detail
MRI • Non-invasive • Soft tissue visualization • Gold standard
MRI • Sagittal images • Visualization of foramen
MYELOGRAPHY • Excellent for intra-canal pathology • Poor for foraminal pathology • Replaced by MRI
MYELOGRAPHY • Invasive • 1% spinal headache • Recurrent stenosis • Inability to obtain MRI
CT-MYELOGRAPHY • Excellent visualization of spinal canal
CT-MYELOGRAPHY • Excellent for recurrent stenosis • Invaluable in surgical planning
MRI • Expensive • Patient cooperation • Claustrophobia • Open MRI
EMG-NCS • Differentiation between neuropathy and radiculopathy • Acute active denervation vs. chronic denervation
NONOPERATIVE RX • Rest • Analgesic • Oral steroid • Physical therapy • Bracing • Spinal injection
REST • Short term activity modification for acute pain • Long term activity modification is not recommended
ANALGESIC • NSAIDS • Tylenol • Narcotics • Neurontin
Oral Steroid • Effective for acute pain • Short duration therapy • ? Chronic or repeat tapering dose
PHYSICAL THERAPY • Avoid extension exercises acutely • William Flexion Exercises • Water aerobics • Strengthening of weak muscle groups
SPINAL INJECTIONS • Epidural steroid • Transforaminal root block • Facet joint injection
EPIDURAL STEROID • Commonly prescribed • 50% short-term efficacy • Not as selective • May not require fluroscope
TRANSFORAMINAL ROOT BLOCK • Highly selective • Diagnostic as well as therapeutic • Delivers medicine to the floor of spinal canal
FACET INJECTION • Facet for back pain • Not for radicular pain • May act as epidural in 40% of cases
SPINAL INJECTION • Most effective for acute pain • May not be indicated in cases of acute denervation or progressive motor loss
OPERATIVE TREATMENT • Decompression of neural element • Stabilization of unstable segment
DECOMPRESSION OF LATERAL RECESS • Undercutting the ventral aspect of the facet joints and the associated ligamentum flavum. • Medial facetectomy if necessary • The traversing nerve root underneath the facet joint must be visualized
FUSION • Sagittal instability • Scoliosis • Iatrogenic pars defect • Greater than 50% facet joint resection