Download
1 / 10
100 likes | 384 Vues
Neuroendocrine tumours of the stomach. Case discussion. Classification. Neuroendocrine tumours of the stomach are rare and are potentially malignant. According to their clinical context they can be divided into three subtypes : 1. tumours in chronic atrophic gastritis ,

E N D
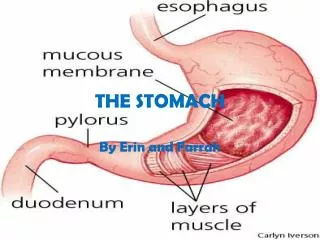
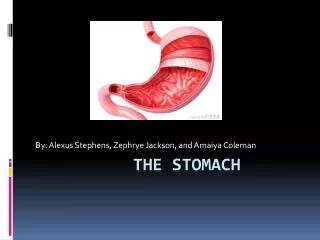
Neuroendocrine tumours of the stomach Case discussion
Classification • Neuroendocrine tumours of the stomach are rare and are potentially malignant. According to their clinical context they can be divided into three subtypes: • 1. tumours in chronic atrophic gastritis, • 2. tumours in multiple endocrine neoplasia type I, • 3. sporadic tumours, not associated with particular diseases. • The first two types may be gastrin-promoted; they occur often multifocal only in the nonantral mucosa and seem to behave relatively benign. Metastasis limited to regional lymph nodes has not been described often. • The very rare third type appears solitary in the whole stomach and seems to have a higher malignant potential with frequent distant metastasis to the liver. Therapy should be mainly guided by subtype and tumour size.
Contd.- Gastric carcinoids • There are three broad groups: • Type 1 - carcinoids associated with chronic atrophic gastritis. • Type 2 - carcinoids associated with the Zollinger-Ellison syndrome. • Type 3 - sporadic gastric carcinoids. • Types 1 and 2 carcinoids are associated with hypergastrinemia. They are usually indolent and metastasis occurs in 10% of cases. They are usually multiple lesions, measuring < 1cm, and can be managed by endoscopic resection with close follow-up endoscopic surveillance. Patients with larger lesions or recurrence may require a partial gastrectomy. Antrectomy results in a decrease in the gastrin levels and may bring about regression of the neoplastic lesions. • Type 3 carcinoids are usually larger (>1 cm) and are more aggressive. Radical gastrectomy is recommended.
Contd.- • As a result of the expansion in our understanding of gastric cellular physiology, knowledge of neuroendocrine tumours of the stomach has increased considerably over the last three decades. In addition, the recognition that neuroendocrine lesions are for the most part confined to the acid-secreting (oxyntic or fundic) mucosa as opposed to the gastrin-secreting (antral or pyloric) mucosa has allowed a distinction to be made between neuroendocrine tumours and adenocarcinomas.
Contd.- • Gastric neuroendocrine tumours are currently classified as • Well differentiated(with enterochromaffin-like (ECL), gastrin-producing (G) and serotonin-producing enterochromaffin (EC) cells as main components) or • Poorly differentiated(large, agressive endocrine carcinomas with poor prognosis) on the basis of the differentiation status of the majority of tumour cells
Contd.- • Deep wall invasion and synchronous metastases are rare events in well-differentiated gastric neuroendocrine tumours. Aggressive behaviour is almost exclusively restricted to Type III ECL-cell tumours and is a typical feature of poorly differentiated endocrine carcinomas (PDEC).
Genetic Studies • Molecular genetic studies on gastric neuroendocrine tumours are scant. • Loss of heterozygosity for microsatellite markers of the 11q13 MEN 1 locus has been identified in a number of gastric neuroendocrine tumours, and has been reported with particularly high frequency in Type II ECL-cell tumours. • Allelic loss of p53 and DCC (deleted-in-colorectal-carcinoma) tumour suppressor genes were identified in both Type III tumours and PDECs. Thus significant genetic differences may exist between gastrin-dependent Type I or II and gastrin-independent Type III ECL-cell tumours and PDECs.
Small cell carcinoma Case Discussion
Dig Dis Sci. 1990 Apr;35(4):513-8. Small cell carcinoma of the stomach. Case report and review of the literature.Hussein AM, Otrakji CL, Hussein BT.Department of Oncology and Pathology, University of Miami Medical School, Jackson Memorial Hospital, Florida 33136.Small cell carcinoma of the stomach is an unusual and rare neoplasm with only eight reported cases in the world literature. Like small cell carcinomas elsewhere, they possess rapid growth ability and high propensity to metastasize with short survival. Clinically, small cell carcinoma is indistinguishable from adenocarcinoma. Because of the rarity of gastric small cell carcinoma, there is minimal information available on the optimal treatment. Herein, we report on a patient with metastatic pure small cell carcinoma of the stomach. He underwent palliative surgery and postoperative combination chemotherapy with transient partial response. He died 10 months after diagnosis with progressive widespread disease.
Gan To Kagaku Ryoho. 2003 Jul;30(7):999-1002.[A case of small cell carcinoma of the stomach]Hasegawa S, Yamamoto Y, Ishiwa N, Yoshikawa T, Morinaga S, Noguchi Y, Matsumoto A.Dept. of Surgery, Kowan Hospital.We report a case of small cell carcinoma of the stomach in a 60-year-old man. The patient was found to have a gastric tumor by routine upper gastrointestinal endoscopy for chronic gastrititis, and was admitted to the hospital. The patient underwent a curative distal gastrectomy with D2 lymph node dissection following a diagnosis of early gastric cancer at the posterior wall of the antrum, in June 2001. Surgical findings were T1, N1, P0, H0, M0, stage I b. The final pathological diagnosis was small cell carcinoma of the stomach with severe lymphatic and vascular invasion (INF alpha, sm, ly3 v2, n1 (+)). In a review of 47 cases seen in the Japanese literature, only 5 patients had early gastric cancer. Lymph node metastasis was observed in 95.0% of all cases, and liver metastasis in 41.0%. Four of the 5 patients with early gastric cancer (80.0%) had lymph node metastases. The prognosis was reported to be extremely poor because small cell carcinoma frequently metastasizes to lymph nodes and/or the liver even in an early stage. The chemotherapy selected by many hospitals is mainly CDDP, but the use of chemotherapeutic drugs varied from hospital to hospital and no effective chemotherapy for the disease has been established as yet.