Download
1 / 1
10 likes | 148 Vues
A Swedish patient registry study examines osteoporosis treatment patterns and quality of life, revealing high-risk patients. Data from 1991-2009 includes clinical assessments and self-reported outcomes.

E N D
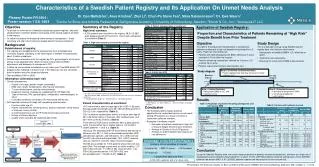
Collection Period:1999 - 2009 Characteristics of a Swedish Patient Registry and Its Application On Unmet Needs Analysis Dr. Dan Mellström1, Arun Krishna2, Zhyi Li3, Chun-Po Steve Fan3, Stina Salomonsson2, Dr. EwaWaern1 1Centre for Bone and Arthritis Research at Sahlgrenska Academy, University of Gothenburg, Sweden; 2Merck & Co., Inc.; 3AsclepiusJT LLC Patient entered registry 2004 Year 2 Year 0 Started collecting EQ-5D in questionnaire Low BMD and/or OP diagnosis Continued follow-up every 2 years if Low BMD and/or OP diagnosis Plenary Poster FR 0404 / Poster session 1 SA 0404 1) Received BMD test 2) Diagnosed for OP 3) Completed questionnaire 1) Received BMD test 2) Diagnosed for OP 3) Completed questionnaire • Objective • To provide an overview of a Swedish osteoporosis patient registry - describe characteristics, treatment patterns and quality of life among subjects enrolled in the registry. • To utilize this registry for analyzing unmet needs of osteoporosis – those remaining at a high risk of fractures despite benefit from prior treatment. • Background • Establishment of registry • The registry was established at the osteoporosis clinic at Sahlgrenska University hospital, Göteborg, in the West region of Sweden encompassing about 2 million inhabitants. • Patients were referred to enter the registry by GPs, gynecologists, etc for dual-energy X-ray absorptiometry (DXA) for bone mineral density (BMD) assessment and diagnosis of osteoporosis (OP) • A follow-up visit would be scheduled in every other year if low BMD and/or OP diagnosis was indicated in the prior visit. If the follow-up visit was cancelled, then the patient would no longer be followed. • Data availability:1991 to 2009. • Information collected at each visit • Clinical assessments: • Patient’s info (age, gender, height, and weight) • BMD scan results (lumbar/spine, total hip and total body) • T-score (lumbar/spine, total hip and total body), • Diagnosis (Normal, Osteopenia, established OP, OP, Male OP) • Type of referrals (GPs, gynecologists, orthopedists, rheumatologists, or other) • Comorbid conditions (secondary OP, rheumatoid arthritis etc) • Self-reported outcomes (through self-completing questionnaire): • Fractures after age 40 • Patient characteristics (smoking status, alcohol, back pain, family history of fractures, history of falls) • Current and previous use of OP treatment and glucocorticoids • History of chronic diseases • Quality of life using EQ-5D (collected after 2004) • Summary of the Registry • High level summary • 9,312 subjects were enrolled in the registry, 38.5% (3,587) were diagnosed with OP and 43.3% (4,031) with osteopenia at enrollment (Table 1) Table 2. Patient characteristics at enrollment Application of Swedish Registry: Normal BMD or no OP diagnosis Normal BMD Or No OP diagnosis • Step 2: (Determine treatment duration) • Patient reported how long they have been treated since last visit Proportion and Characteristics of Patients Remaining at “High Risk” Despite Benefit from Prior Treatment Baseline (Visit 1) 2nd visit (Visit 2) Treatment ≥ 2 years Patient exit registry Patient exit registry Table 1. High level summary counts of the registry • Objective • To examine the proportion/characteristics of osteoporotic patients remaining at a high risk despite being treated for ≥ 2 years. “High risk” was defined as: • Patients with deteriorating/worsen BMD, defined as T-score decrease ≥ 3% at either hip or spine • Patients remaining osteoporotic, defined as T-score ≤ -2.5 at either hip or spine • Patients experienced fracture after baseline visit • Study Design • This is a descriptive study using Swedish patient registry data, the inclusion criteria were: • Osteoporotic at baseline (BMD≤ -2.5, either hip or spine) • Treatment naïve at baseline • Returned for a 2nd visit for BMD measurements • Step 1: (Patient Selection) • Osteoporotic (BMD ≤-2.5), and • Treatment naïve • Step 3: (Outcome measures) • % with deteriorating/worsen BMD • % remaining osteoporotic • % with fracture • Study diagram Table 3. EQ-5D (N=1,570) * Only those with complete response to all EQ-5D questions ** EQ-5D started on 2004, therefore the first measurement was not necessary recorded at enrollment *** Including “Fibrous dysplasia”, “Skeletal fluorosis”, “other bone disorder” Results Responses to each of the 5 EQ-5D questions 1 = No Problem , 2 = Some Problem, 3 = Extreme Problem or Not Able to Perform • Patient characteristics at enrollment • 91% were female, with average age of 64.1 [SD=11.8] years. Average weight and height were 66.1 [SD=20.6] kg and 161.4 [SD=22.3] cm, respectively. (Table 2) • 23% of patients reported prior history of fracture after age 40, 35% had family history of fractures, 28% had back pain, and 33% were currently smokers. (Table 2) • From the first DXA scan at enrollment, 36% (3,292) patients had a T-score (either hip or lumbar spine) ≤ -2.5 and 42% (3,897) between -1 and -2.5. (Table 2) • Among 2,101 diagnosed with OP at enrollment and having ≥1 follow-up visit, 55% (1,146) received bisphosphonates (BIS) (alendronate, optinate, and etidronate), 12% (259) received non-BIS (raloxifene and teriparatide), 79% (1,651) received calcium+vitamin D, and 26% (542) received estrogen. • EQ-5D was available for 1,570 patients whose first visit was post-2004. The average scores were as follow: mobility: 1.37 [SD=0.49], self-care: 1.11 [SD=0.35], usual activities: 1.34 [SD=0.56], pain/discomfort: 1.91 [SD=0.60], and anxiety/depression: 1.52 [SD=0.57]. (Table 3) Table 4. Proportion of patients remaining osteoporotic and with worsen BMD Table 5. Fracture and treatment received • Conclusion • The Swedish patient registry presents opportunities to understand various unmet needs among OP patients as a result of extensive information collected overtime. • Examples of analyses include: • Estimation of patients remained at “highrisk” of fracture despite benefit of prior treatment • Analysis of Quality of life of OP patients • Analysis of under-treatment and reasons for non-adherence Follow-up visit • Conclusion • Using the Swedish Registry data, we found a large proportion of patients remained osteoporotic, and were at a high risk of developing fractures despite being treated for ≥ 2 years. 75.8% (297/392) patients remained osteoporotic, 23.0% (90/392) patients had worsen BMD, 5.9% (23/392) patients experienced fracture prior to their second visit. Subjects were invited for a follow-up visit every 2 years if the prior visit showed low BMD/OP diagnosis Presented at The American Society for Bone and Mineral Research (ASBMR) 2013 Annual Meeting, Baltimore, MD, October 4 – 7, 2013