Download
1 / 69
710 likes | 1.18k Vues
Chapter 18 Analysis and Monitoring of Gas Exchange. Learning Objectives. Describe the difference between monitoring and analysis. Describe the two types of electrochemical oxygen analyzers. Describe calibration and problem-solving techniques for oxygen analyzers.

E N D
Learning Objectives • Describe the difference between monitoring and analysis. • Describe the two types of electrochemical oxygen analyzers. • Describe calibration and problem-solving techniques for oxygen analyzers. • State how to obtain, process, and analyze arterial and capillary blood gas samples. • List the quality control procedures applied to blood gas analysis.
Learning Objectives (cont.) • List the potential advantages of point-of-care testing. • Describe how to obtain and interpret transcutaneous oxygen and carbon dioxide monitoring. • Describe the basic principles used by an oximeter to monitor oxygen saturation. • State when and how to perform pulse oximetry. • Identify true statements related to interpretation of pulse oximetry results. • Describe how to perform capnometry and interpret capnograms.
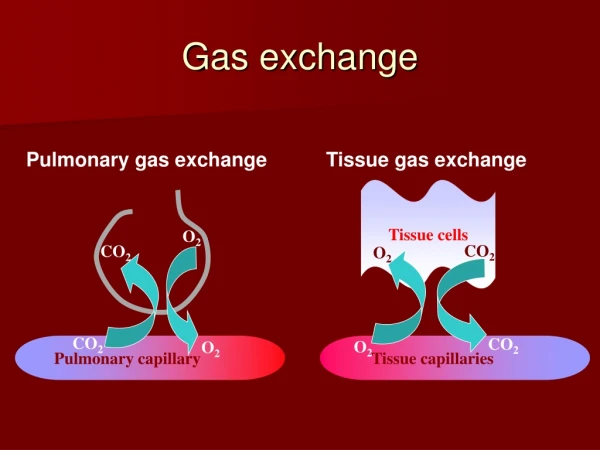
Analysis vs. Monitoring Laboratory analysis: discrete measurements of fluids or tissue that must be removed from body Such measurements are made with an analyzer Monitoring is an ongoing process by which clinicians obtain & evaluate dynamic physiological processes in a timely manner, usually at bedside This is done with monitor
Invasive vs. Noninvasive Procedures Invasive procedures require insertion of sensor or collection device into body Noninvasive monitoring is means of gathering data externally Generally, invasive procedures provide more accurate data but carry greater risk After gradient between invasive & noninvasive method is established, trends in change of noninvasive method can be useful in making clinical decisions
Measuring FIO2 • Most bedside systems to measure FIO2 use electrochemical principles • 2 most common: • Polargraphic (Clark) electrode- needs battery • Galvanic fuel cell- no battery needed • Response times for Clark electrodes = about 10 to 30 seconds • Response times for galvanic fuel cells = 60 seconds
Working as a new therapist in the ICU you come across an O2 analyzer that uses battery to only power its alarm system. This analyzer should be classified as a: • paramagnetic analyzer • polarographic analyzer • galvanic fuel cell analyzer • zirconum cell analyzer
Troubleshooting O2 Analyzers • Calibration according to manufacturer’s recommendation must be done before using device • Failure to calibrate or inconsistent readings are signs of malfunctioning • Best way to avoid problems is through preventative maintenance • If analyzer fails to calibrate, problem could be related to: • Low batteries, sensor depletion, electronic failure
All of these may be reasons for a Galvanic fuel cell to malfunction, except: • batteries • sensor depletion • electric failure • condensation of water vapor
Sampling & Analyzing Blood Gases • Analyzing arterial blood samples is important part of diagnosing & treating patients with respiratory failure • Radial artery is most often used because: • Near surface & easy to stabilize • Collateral circulation usually exists (confirmed with the Allen test) • No large veins are near • Radial puncture is relatively pain free • Arterial cannulation can be done if frequent sampling is needed
Arterial Sampling (cont.) • Modified Allen’s test: • Done prior to radial artery puncture ONLY • Normal test indicating collateral circulation - hand flush pink within 5-10 seconds • Cannot be performed on critically ill patients who are uncooperative or unconscious
The RT receives a doctor order to perform an ABG on a 32 year-old patient. Prior to performing the ABG, the RT does a modified Allen’s test on the patient’s right hand that takes more than 10 seconds for patient’s hand to flush pink. What should the RT do next? • should not perform an ABG on patient. • perform the ABG on the right brachial artery. • perform it on the right radial artery. • repeat the modified Allen’s test on the left hand.
Arterial Sampling (cont.) • Sample volume of 0.5 to 1 mL of blood is adequate • Actual volume depends on: • Anticoagulant used • Requirements of specific analyzer used • Whether or not other tests will be performed on obtained sample
Arterial Sampling (cont.) • Important transmission-based and safety precautions: • Never recap used needle without safety device; never handle using both hands, & never point it toward any part of body • Never bend, break, or remove used needles from syringes by hand • Always dispose of used syringes, needles, & other sharp items in appropriate puncture-resistant sharps containers
Indications for Arterial Sampling Sudden, unexplained dyspnea Acute shortness of breath/tachypnea Abnormal breath sounds Cyanosis Heavy use of accessory muscles Changes in ventilator settings CPR Diffuse infiltrates in chest radiograph New infiltrates in CXR Sudden cardiac arrhythmias Acute hypotenesion
Blood Sample Analysis • Clinicians can avoid most pre-analytical errors by ensuring that sample is: • Obtained anaerobically • Properly anticoagulated • Analyzed within 10 to 30 minutes
Interpretation of ABGs • Interpret oxygenation status • PaO2 (see below) • SaO2 (normal = 95100%) • CaO2 (normal = 1820 vol%) • PaO2 6079 mm Hg = mild hypoxemia • PaO2 4059 mm Hg = moderate hypoxemia • PaO2 <40 mm Hg = severe hypoxemia
The RT is called to run an ABG drawn by the unit resident on a patient in a non-rebreather mask. The RT notices visible bubbles at the top of the blood sample. How this may impact the PaO2 and PaCO2 results? • it may increase the PaCO2 of the sample • it only affects the gas pressures after 1 hr of drawn • it may decrease the PaO2 of the sample • air bubbles have no impact on the PaO2/PaCO2 values
Indwelling Catheters • Provides ready access for blood sampling • Allow continuous monitoring of vascular pressures • Infection & thrombosis are more likely than intermittent punctures • Normal routes are peripheral arteries (radial, brachial, pedal), femoral artery, central vein, & pulmonary artery
Indwelling Catheter (cont.) • Access for sampling blood from most intravascular lines is provided by a three-way stopcock • Pulmonary artery catheter has separate blood sampling and IV infusion ports and balloon at tip
If a indwelling vascular catheter is placed in the brachial artery, what is the sample assessing? • pulmonary gas exchange • gas exchange at the tissues • right ventricular preload • right ventricular afterload
Capillary Blood Gases Good capillary sample can accurately reflect & provide clinically useful estimates of arterial pH & PCO2 levels Capillary PO2 is of no value in estimating arterial oxygenation. SaO2 must be evaluated by pulse oximetry. Most common technical errors in capillary sampling are inadequate warming & squeezing of puncture site Squeezing puncture site may result in venous & lymphatic contamination of sample
Analyzing • Measures pH, PCO2, & PO2 levels in blood sample • Several secondary values are calculated: • Plasma • Bicarbonate (HCO3-) • Base excess (BE) or deficit • Hemoglobin saturation (HbO2%). • Some may combine blood gas & hemoximetry (total hemoglobin) measurements
Instrumentation • Can be based on several different types of sensor technology to measure pH, PCO2, & PO2: • Electrochemical electrodes • Optical fluorescence • Photoluminescence
Instrumentation (cont.) • Electrodes: • PaO2: Clark polarographic electrode • PaCO2: Severinghaus electrode • pH: pH electrode actually consists of 2 electrodes or half-cells: • Measuring electrode • Reference electrode
Quality Assurance • Accurate ABG results depend on rigorous quality control efforts • Components of quality control are: • Record keeping (policies & procedures) • Performance validation (testing new instrument) • Preventative maintenance & function checks • Automated calibration & verification • Internal statistical quality control • External quality control (proficiency testing) • Remedial action (to correct errors)
Quality Control Components • Recordkeeping • Performance Validation • Preventive maintenance and function checks • Automated calibration • Calibration verification by control media • Internal statistical quality control • External quality control • Remedial actions
Changes on procedures, staff training and retraining, closer supervision and increase in maintenance checks are an example of which of the following quality control elements? • external quality control • remedial action • calibration verification • performance validation
Point-of-Care Testing • Performing blood gas analysis from laboratory to patient’s bedside • Reduces turnaround time, thus should improve care & lower costs • Used increasingly in hospitals & physician offices • Used for blood chemistry & hematology parameters
Blood Gas Monitoring • Provides continuous or interval measurements without removing blood from patient • 4 systems in current clinical use: • Transcutaneous blood gas monitor • Intra-arterial (in-vivo) blood gas monitor • Extra-arterial (ex-vivo) blood gas monitor • Tissue oxygen monitor
Transcutaneous Monitoring Provides continuous, noninvasive estimates of PO2 and PCO2 using skin sensor Sensor warms underlying skin to increase arterial blood flow 2 most important factors influencing accuracy of transcutaneous measurements: age & perfusion status Low perfusion & increasing age reduce agreement between PtcO2 & PaO2 Agreement between PtcCO2 & PaCO2 is better because CO2 is more diffusible through skin
Transcutaneous Monitoring (cont.) • Most common sites for electrode placement for infants & children are abdomen, chest & lower back • Should compare monitor readings with those obtained with concurrent ABG • Validation with ABG should be repeated anytime patient’s status undergoes major change
Current data in an infant reveals a PTCO2 of 98 mm Hg and a PTCO2 of 22 mm Hg. A stat ABG is ordered showing a PaO2 of 56 mm Hg and a PaCO2 of 49 mm Hg? What could be the cause of this discrepancy? • an air leak • electrode placement • decreased skin perfusion • electrode overheating
Intra-arterial (In Vivo) • Potential benefits of continuous blood gas analysis: • Real time monitoring • Reduction in therapeutic decision making time • Less blood loss • Lower infection risk • Improved accuracy • Elimination of specimen transport
Extra-arterial (Ex Vivo) • Eliminates all problems associated with indwelling sensors • Provides quick results • Unable to provide real-time continuous data • Determine further justification of costs & patient benefits
Tissue Oxygen (PtO2) Monitor • Tissue oxygen can be measured by probes inserted directly into organs, tissue, & body fluids • Clinical indications: • Monitor brain tissue oxygen as an early sign of ischemia • Assess brain blood flow autoregulation • Monitor adequacy of brain perfusion in patients with traumatic brain injury
Factors that affect transcutaneous blood gas monitoring accuracy includes all of the following, except: • variation in skin characteristics • temperature • electrode placement • hematocrit
Oximetry Oximetry measures hemoglobin saturation using spectrophotometry Oximetry works because each substance has its own unique pattern of light absorption Each form of hemoglobin (e.g., HbO2, HbCO) has its own pattern of light absorption For example, HbO2 absorbs less red light & more infrared light