Download
1 / 12
120 likes | 136 Vues
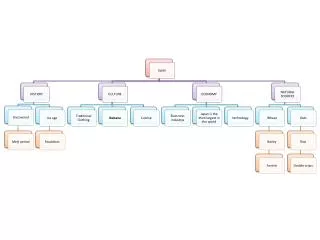
Learn how to use concept maps to guide nursing care documentation and understand the relationships between ANA standards, documentation standards, and concept map care plans.

E N D
Objectives • List purposes of documentation • Describe the relationships between the ANA standards of care, ANA documentation standard, and concept map care plan. • Specify the basic content of nursing care documentation
Objectives • Compare documentation formats for standardized forms and narrative progress notes • Identify basis criteria that guide documentation • Use the concept map care plan to identify content for documentation
What is “Documentation”? It is the legal record of written communication of all patient careactivities. -Individual client -Group of clients
Purpose of Documentation • To facilitate communication • To promote good nursing care • To meet professional and legal standards
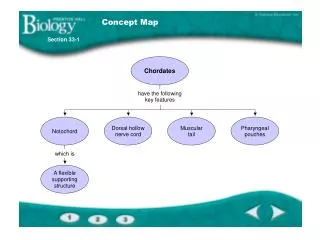
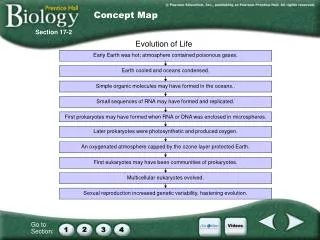
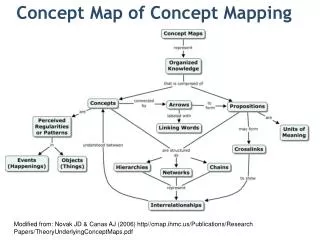
What to Documentation ? Everything on the map needs to be documentation somewhere!!
ANA Standard of Care • Standard 1: Assessment • Standard 2: Diagnosis • Standard 3: Outcome Identification • Standard 4: Planning • Standard 5: Implementation • Standard 6: Evaluation
Tool for Documentation • Worksheets and kardexes • Client care plans • Flow sheets and checklists • Care maps and clinical pathways • Monitoring strips
Documentation Method • Focus charting Data, Action, Response • “SOAP” charting • Narrative charting
Documentation of Specific Problem For each nursing diagnosis, documentation can be done in three steps that are as easy as “ PIE”. Problem Intervention Evaluation patient responses
Accuracy Legibility Signature Correcting mistakes Logical organization of information Writing a late entry Completeness Omitted intervention Conciseness Note concerning other health-care providers How to Documentation