Download
1 / 110
1.11k likes | 1.29k Vues
Explore normal CT anatomy of the digestive system and identify key structures such as hepatic veins, portal veins, and adrenal glands. Learn about gallstones, kidney stones, calcified adrenal glands, and bowel obstructions. Discover the radiographic patterns of esophageal carcinoma.

E N D
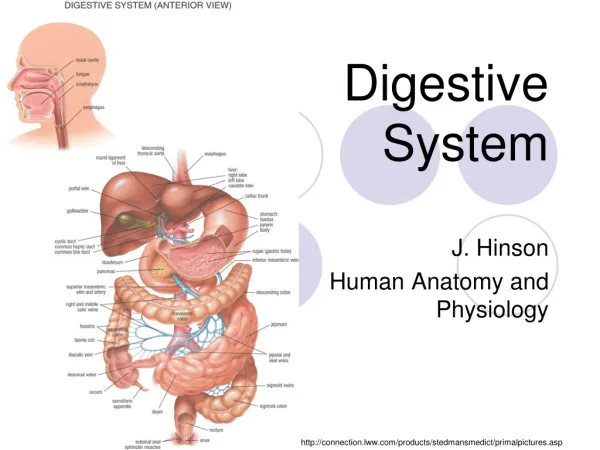
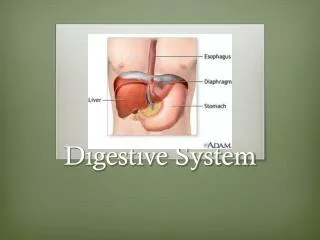
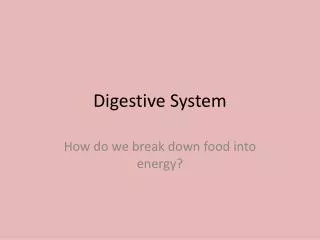
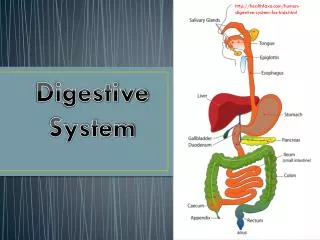
Radiology of Digestive System Department of Radiology Zhongshan Hospital, Fudan university RAO Sheng-Xiang
Plain film radiograph • Hepatic angle • Spenic angle • Renal shadow • Psoas muscle • Properitoneal fat strip
Normal CT anatomy 1.LHV, left hepatic vein 2.MHV, middle hepatic vein; 3.RHV, right hepatic vein; 4.IVC, inferior vena cava 5.Ao,aorta 6.Stomach 1 2 4 6 3 5
1.LPV, left portal vein 2.Stomach 3.Speen 4.IVC, inferior vena cava 5.Ao,aorta 1 2 4 5 3
1.Gallbladder 2.RPV, right portal vein 3.antrum 4.duodenal bulb 3 1 4 1
1.CA,celiac axis 2.Splenic artery 3.common hepatic artery 4.Duodenum 5.Kidney 6.Pancreas 7.Portal vein 8.Adrenal gland 2 6 7 3 1 4 5 5
SMA:superior mesenteric artery • CBD,common bile duct • Spenic vein • Pancreas
SMV, superior mesenteric vein • SMA, superior mesenteric artery • Uncinate process
CTA • SMA, superior mesenteric artery • CA,celiac axis • Splenic artery • common hepatic artery
main portal trunk; • right portal branch; • splenic vein; • inferior mesenteric vein; • superior mesenteric vein
RHV, right hepatic vein; • MHV, middle hepatic vein; • LHV, left hepatic vein • IVC, inferior vena cava
Upper abdominal calcification • may be an important sign of disease • Gallstones ,Porcelain gallbladder • Urinary Calculi • Calcified adrenal glands • Pancreatic calcification • Tumor calcification • ……………
Gallstones • 15% -20%of gallstones contain sufficient calcium to be identified on plain film • right upper quadrant • laminated appearance (a dense outer rim and more radiolucent center)
Porcelain gallbladder • calcification in the wall of the gallbladder • indicative of chronic obstruction of the cystic duct, chronic gallbladder inflammation, and an increased risk of gallbladder carcinoma
Discontinuous mural calcification diffuse
Kidney stones • About 85% of urinary calculi are visible on plain film. • Staghorn Calculus a large calculus occupying the collecting system of the left kidney and assuming its shape
Calcified adrenal glands • associated with adrenal hemorrhage in the newborn, tuberculosis, and Addison disease • either side of the first lumbar vertebra
Pancreatic Calcifications • chronic alcohol-induced pancreatitis • Coarse and punctate calcifications • extend upward across the left upper quadrant
Intestinal Distention • The small bowel is dilated when it exceeds 2.5 to 3.0 cm in diameter. • The colon is dilated when it exceeds 5 cm in diameter • The cecum is dilated when it exceeds 8 cm in diameter.
Normal Bowel Gas Pattern • The normal distribution of gas in the stomach and duodenum • The colon----- mottled pattern of stool • The small bowel----a few gas collections
Mechanical bowel obstruction Small Bowel • Dilated loops of small bowel (>3 cm) • Air-fluid levels that exceed 2.5 cm in length • Air-fluid levels at differing heights within the same loop (strong evidence of obstruction) • Small bubbles of gas trapped between the valvulae conniventes
Erect radiograph of the abdomen • Air-fluid levels at different heights • The valvulae conniventes that extend across the entire diameter of the bowel lumen
Mechanical bowel obstruction Large Bowel • Most colonic obstructions occur in the sigmoid colon • Dilation of the colon from the cecum to the point of obstruction • The colon distal to the obstruction is devoid of gas
Sigmoid volvulus • A large gas-filled loop(inverted U shape or a coffee bean shape) without haustra or septa, • Arising from the pelvis and extending high into the abdomen and often to the diaphragm • Barium enema: a beaking sign at the point of the twist
Adynamic ileus(Functional ileus) • Decreased or absent peristalsis • Diffuse gaseous, distension of bowel(small bowel and colon,rectum)
Pneumoperitoneum • Common causes:bowel perforation, trauma, recent surgery • Free air beneath the domes of the diaphragm
Dysphagia: Esophagus • The length of the esophagus is tubular, and its termination is saccular • A ring: the tubulovestibular junction is formed by a symmetric muscular ring • B ring : an asymmetric mucosal ring or notch that occurs at the junction of esophageal squamous epithelium with gastric columnar epithelium
The esophageal vestibule demarcated by the muscular A ring and the mucosal fold of the B ring • B ring (mucosal ring) <14mm---always symptomatic 14mm-20mm--50% symptomatic >20mm---asymptomatic
Benign Stricture Resulting from Reflux Esophagitis • usually confined to the distal esophagus • may be tapered, smooth, and circumferential (the classic appearance)
Esophageal carcinoma Four basic radiographic patterns • An annular constricting lesion, appearing as an irregular ulcerated stricture, is most common. • The polypoid pattern causes an intraluminal filling defect • The infiltrative variety grows predominantly in the submucosa and may simulate a benign stricture. • The least common pattern is that of an ulcerated mass.
Malignant Stricture • Abrupt narrowing with irregular mucosa • The prominent shoulders are characteristic of tumor
Esophageal achalasia • usually at age 30 to 50 years • Absence of peristalsis of body of esophagus • Failure of the LES to relax with swallowing • Smooth,tapered or beaklike appearance
Normal anatomy of stomach • composed of the cardia, fundus, body, and antrum
A well-distended stomach has a wall thickness of approximately 5 mm
Benign Ulcer(1) • Projection beyond the lumen of stomach • soomth lucent line (collar ) at the neck of ulcer
Benign Ulcer(2) Hampton line :a thin, sharp, lucent line that traverses the orifice of the ulcer.
Benign Ulcer(3) Radiating folds extending into the crater
Malignant ulcer • location within the lumen of the stomach • nodular, rolled, irregular, or shouldered edges
Gastric adenocarcinoma • The most common malignancy in the stomach • The pattern of spread : local extension , distant metastases drop metastases to the ovaries
Polypoid Gastric Carcinoma. a lobulated filling defect (arrows) in the antrum of the stomach.
CT: • focal wall thickening • diffuse wall thickening • a lobular mass with or without ulceration • destruction of the multilayered pattern or with transmural enhancement • regional lymphadenopathy; metastases