Download

1 / 69
720 likes | 987 Vues
Trial Comparison: ‘Arimidex’, Tamoxifen, Alone or in Combination (ATAC) and Breast International Group (BIG) 1-98. Trial design and patient recruitment. Netherlands 195 Poland 107 Portugal 74 Slovakia 33 Spain 417 Sweden 291 Turkey 53 UK 3228. Belgium 192 Czech Republic 84

E N D
Trial Comparison: ‘Arimidex’, Tamoxifen, Alone or in Combination (ATAC) and Breast International Group (BIG) 1-98
Netherlands 195 Poland 107 Portugal 74 Slovakia 33 Spain 417 Sweden 291 Turkey 53 UK 3228 Belgium 192 Czech Republic 84 France 366 Germany 121 Hungary 243 Ireland 41 Italy 654 640 2222 160 30 201 14 9366 patients recruited from 381 centres in 21 countries ATAC trial:
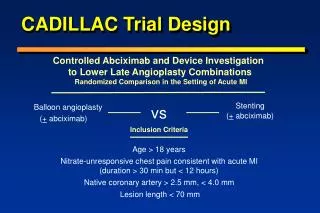
Combination n=3125 ATAC trial design 9366 postmenopausal women with invasive breast cancer: mean age 64 years; 84% hormone receptor-positive; 61% node negative; 64% with tumour 2 cm in diameter Surgery radiotherapy chemotherapy Randomisation 1:1:1 for 5 years Discontinued following initial analysis as no efficacy or tolerability benefit compared with tamoxifen arm Anastrozole n=3125 Tamoxifen n=3116 Regular follow-up • Secondary trial endpoints: • Incidence of contralateral breast cancer • Time to distant recurrence • Overall survival • Time to breast cancer death • Primary trial endpoints: • Disease-free survival • Safety / tolerability
ATAC Completed Treatment Analysis • Data cut-off 31 March 2004, based on at least 704 deaths in the two monotherapy arms combined • 68 months’ median follow-up – beyond completion of treatment • 59 months’ median treatment duration • Only 8% of patients remain on treatment – the great majority of these nearing completion ATAC Trialists’ Group. Lancet 2005; 365: 60-62
BIG 1-98 trial design R A N D O M I S E Arm Tamoxifen A 8028 postmenopausal women with ER+ diseaseMedian age 61 years52% node negative63% tumour 2 cm in diameter B Letrozole Tamoxifen Letrozole C Letrozole Tamoxifen D 0 1 2 3 4 5 Time (years) A vs B: March 1998 – March 2000; (n=1835) A vs B vs C vs D; September 1999 – May 2003; (n = 6193) BIG = Breast International GroupER+ = estrogen receptor-positive Adapted from Thürlimann B. St Gallen presentation 2005
ATAC: 73% of patients have been followed-up for 5 years or more Patients (%) Updated analysis (median follow-up 47 months) Treatment completion analysis (median follow-up 68 months) <1 1–<2 2–<3 3–<4 4–<5 >5 Duration of follow-up (years) Total number of DFS events (monotherapy arms) 1226 DFS = disease-free survival
BIG 1-98: only 15% of patients have been followed-up for 5 years Patients (%) 1 2 3 4 5 Follow-up (years) Thürlimann B. St Gallen presentation 2005
Patient characteristics ATAC (n=6291) BIG 1-98 (n=8010) Age (years) Primary treatment (%) mastectomy radiotherapy chemotherapy Mean64.1 47.6 62.9 21.6 Median61.0 43.0 71.6 25.3 ATAC Trialists’ Group. Lancet 2002; 359: 2131-39Adapted from Thürlimann B. St Gallen presentation 2005
Baseline disease characteristics ATAC (n=6291) BIG 1-98 (n=8010) Tumour size 2 cm (%) Nodal status (%) node-positive node-negative unknown HR status (%) ER+/PgR+ ER+/PgR- ER+/PgR unknown ER-/PgR+ 63.4 34.2 60.7 5.0 61.5 14.1 5.5 2.2 62.9 41.3 52.2 6.5 63.1 20.4 14.4 1.8 ATAC Trialists’ Group. Lancet 2002; 359: 2131-39Adapted from Thürlimann B. St Gallen presentation 2005
Definition of disease-free survival differs • ATAC • loco-regional recurrence or new contralateral breast cancer (invasive or DCIS) • distant recurrence or death (for any reason) • BIG 1-98 • breast cancer recurrence (local, regional and distant) or invasive contralateral breast cancer • non-breast cancer deaths (deaths without recurrence) • non-breast cancer second primaries • Time to recurrence is similar for both trials ATAC Trialists’ Group. Lancet 2002; 359: 2131-39Thürlimann B et al. The Breast 2005;14; S3. Abstract S4 DCIS = ductal carcinoma in situ
Definition of time to distantrecurrence appears to differ • ATAC - time to distant recurrence (TTDR) • distant recurrence or any death following a loco-regional recurrence (including ipsilateral new breast cancer) or breast cancer death • ~45% of first events were distant events • ~18% of first events were locoregional • BIG 1-98 - time to distant metastasis (TTM) • breast cancer recurrence (excluding local or regional recurrences, and contralateral breast cancer) • censoring for non-breast cancer deaths • ~65% of first events* were distant events • ~12% of first events* were local or regional ATAC Trialists’ Group. Lancet 2005; 365: 60-62Thürlimann B et al. The Breast 2005;14; S3. Abstract S4 *excluding second primary events
Anastrozole (A) Tamoxifen (T) ATAC: disease-free survival (HR-positive population) Patients(%) 25 HR 0.83 95% CI (0.73, 0.94) p value 0.005 A vs T 20 15 10 5 1.6% 2.6% 2.5% 3.3% Absolute difference: 0 0 1 2 3 4 5 6 Follow-up time (years) At risk: A 2618 2540 2448 2355 2268 2014 830 T 2598 2516 2398 2304 2189 1932 774 Howell A. SABCS presentation 2004 CI, confidence interval
BIG 1-98: disease-free survival Yearly 97.7 95.1 90.5 86.8 84.0 L DFS % 97.6 93.4 89.0 84.6 81.4 T HR 0.81 95% CI (0.70, 0.93) p value 0.003 L vs T 25 20 N=8010 15 10 Letrozole Tamoxifen 5 0 0 1 2 3 4 5 Follow-up time (years) At risk: 4003 3892 2964 1261 892 567 L 4007 3896 2926 1238 866 544 T Adapted from Thürlimann B. St Gallen presentation 2005
Anastrozole (A) Tamoxifen (T) ATAC: recurrence (HR-positive population) Patients(%) 25 p value 0.0002 HR 0.74 95% CI (0.64, 0.87) A vs T 20 15 10 5 1.7% 2.4% 2.8% 3.7% Absolute difference: 0 0 1 2 3 4 5 6 Follow-up time (years) At risk: A 2618 2540 2448 2355 2268 2014 830 T 2598 2516 2398 2304 2189 1932 774 ATAC Trialists’ Group. Lancet 2005;365:60-62
BIG 1-98: breast cancer relapse(Time to recurrence)Cumulative incidence 20 Proportion failure (%) 5-year difference (L-T) = -3.41.2% p=0.0002 (based on CI) 13.6% 15 Letrozole (L) Tamoxifen (T) 8.1% 10 10.2% 5 6.2% 0 0 1 2 3 4 5 Years from randomisation Thürlimann B. St Gallen presentation 2005
Anastrozole (A) Tamoxifen (T) ATAC: time to distant recurrence (HR-positive population) Patients(%) 25 p value 0.06 HR 0.84 95% CI (0.70, 1.00) A vs T 20 15 10 5 0 0 1 2 3 4 5 6 Follow-up time (years) At risk: A 2618 2550 2464 2386 2309 2051 845 T 2598 2533 2438 2361 2251 2005 816 Howell A. SABCS presentation 2004
Anastrozole (A) Tamoxifen (T) ATAC: overall survival (HR-positive population) Patients(%) 25 p value 0.7 HR 0.97 95% CI (0.83, 1.14) A vs T 20 15 10 5 0 0 1 2 3 4 5 6 Follow-up time (years) At risk: A 2618 2566 2505 2437 2377 2117 867 T 2598 2549 2502 2430 2333 2080 855 Howell A. SABCS presentation 2004
ATAC: efficacy summary(HR-positive population) Hazardratio Disease-free survival 0.83 Time to recurrence 0.74 Time to distant recurrence 0.84 Overall survival 0.97 Time to breast cancer death 0.87 Contralateral breast cancer 0.47 0.2 0.4 0.6 0.8 1.0 1.2 2.0 1.5 Hazard ratio (A:T) and 95% CI Anastrozole (A) better Tamoxifen (T) better ATAC Trialists’ Group. Lancet 2005;365:60-62
ATAC: efficacy analysis (ITT and HR +ve) ITT HR+ 0.83 0.74 0.84 0.97 0.87 0.47 0.87 0.79 0.86 0.97 0.88 0.58 Disease-free survival Time to recurrence Time to distant recurrence Overall survival Time to breast cancer death Contralateral breast cancer 0.2 0.4 0.6 0.8 1.0 1.2 1.5 2.0 HR (A:T) and 95% CI ITT population Anastrozole (A) better Tamoxifen (T) better HR +ve population ATAC Trialists’ Group. Lancet 2005;365:60-62
BIG 1-98: efficacy summary Hazard ratio BIG 1-98 ATAC Disease-free survival 0.81 Time to recurrence 0.72 0.74 Time to distant recurrence 0.73 0.84 Overall survival 0.86 0.97 Systemic disease-free survival 0.83 Disease-free survival (without 2nd primary) 0.79 0.83 0.2 0.4 0.6 0.8 1.0 1.2 2.0 1.5 Hazard ratio (L:T) and 95% CI Letrozole (L) better Tamoxifen (T) better Adapted from Thürlimann B. St Gallen presentation 2005
BIG 1-98: sites of first failure Letrozole (%) Tamoxifen (%) p value Failures (DFS events) local contralateral breast regional* distant second (non-breast) malignancy death without recurrence Deaths Systemic failures** 8.8 0.5 0.4 0.3 4.4 1.7 1.4 4.1 8.1 10.7 0.9 0.7 0.3 5.8 2.0 0.9 4.8 9.6 0.004 0.047 0.125 0.845 0.006 0.324 0.077 0.176 0.020 *Regional includes axilla or internal mammary**SDFS ignores local and contralateral events Thürlimann B. St Gallen presentation 2005
ATAC vs BIG 1-98 efficacy summary • Anastrozole is more effective than tamoxifen in reducing the risk of recurrence, distant recurrence and contralateral breast cancer • absolute difference between anastrozole and tamoxifen continues to increase over time, and extends beyond completion of treatment • Letrozole demonstrates DFS benefits and early benefits in distant recurrence • BIG 1-98 has a comparatively higher number of patients per arm, resulting in a higher number of events per unit time • patient population in BIG 1-98 has a slightly worse prognosis • Absolute differences at 5 years for BIG 1-98 data are projected out to 5 years and are calculated from immature data hence liable to change
Nodal status +ve -ve Tumour size ≤2 cm >2 cm Receptor status +ve -ve Previous chemotherapy yes no ATAC: time-to-recurrence by subgroup All patients 0.40 0.60 0.80 1.00 1.25 1.50 1.75 Intent-to-treat population Hazard ratio (A:T) and 95% CI Anastrozole (A) better Tamoxifen (T) better Howell A. SABCS presentation 2004
Nodal status +ve -ve Previous chemotherapy Previous radiotherapy yes no yes no BIG 1-98: disease-free survivalby subgroup All patients 0.40 0.60 0.80 1.00 1.25 1.50 1.75 Intent-to-treat population Hazard ratio (L:T) and 95% CI Letrozole (L) better Tamoxifen (T) better Adapted from Thürlimann B. St Gallen presentation 2005
ATAC vs BIG 1-98 subgroup summary (1) • Anastrozole demonstrated advantages over tamoxifen for all subgroups examined • no heterogeneity of subgroups • no significant interaction with any baseline prognostic factor, including prior chemotherapy or nodal status • more effective than tamoxifen in overall HR+ve group • even greater improvement in ER+PgR- subgroup • Subgroup analyses must be interpreted with caution • should not be used as a basis for making clinical decisions
ATAC vs BIG 1-98 subgroup summary (2) • Letrozole demonstrated benefits over tamoxifen • node positive patients • no apparent benefit in node negative patients • prior chemotherapy patients • slightly worse prognosis, more patients received prior chemotherapy (25% vs 20%) • No apparent difference between ER+/PgR+ and ER+/PgR- subgroups for letrozole and tamoxifen • tamoxifen does not appear to be performing in line with expectations • previous studies demonstrate that ER+/PgR- patients on tamoxifen have a higher rate of recurrence than ER+/PgR+ • Subgroup analyses must be interpreted with caution • should not be used as a basis for making clinical decisions
BIG 1-98: safety analysis • Included all patients that had received at least 1 treatment dose • Protocol-specified only ‘targeted’ adverse event data was collected every 6 months • Number of patients experiencing at least 1 serious adverse event: • 587 vs 643 (letrozole vs tamoxifen)
ATAC: overview of adverse events* All adverse events Adverse events leading to withdrawal Drug-related adverse events leading to withdrawal All serious adverse events Serious adverse events leading to withdrawal Serious adverse events leading to death Drug-related serious adverse events leading to death Anastrozole (%)(n=3092) 93.9 11.1 6.5 33.3 4.7 3.3 0.2 Tamoxifen (%)(n=3094) 94.6 14.3 8.9 36.0 5.9 3.6 0.3 p value 0.2 0.0002 0.0005 0.03 0.04 0.6 0.5 Howell A. SABCS presentation 2004 *Adverse events on treatment or within 14 days of discontinuation
ATAC: pre-defined adverse events* Completion analysis (%) p value A 35.7 5.4 3.5 0.2 2.0 2.8 1.6 35.6 11.0 T 40.9 10.2 13.2 0.8 2.8 4.5 2.4 29.4 7.7 <0.0001 <0.0001 <0.0001 0.02 0.03 0.0004 0.02 <0.0001 <0.0001 Hot flushes Vaginal bleeding Vaginal discharge Endometrial cancer** Ischaemic cerebrovascularevent Venous thromboembolicevents Deep venous thromboembolic events Joint symptoms Total fractures*** *Adverse events on treatment or within 14 days of discontinuation; **Excludes patients with prior hysterectomy and includes on- and off-therapy AEs; ***Fractures occurring at anytime prior to recurrence (includes patients no longer receiving treatment) ATAC Trialists’ Group. Lancet 2005;365:60-62
BIG 1-98: targeted adverse events Primary core analysis (%) L 33.6 3.3 14 8.8 1.0 2.7 1.2 8.7 5.8 43.6 T 38.1 6.6 16.2 9.5 2.4 2.6 1.1 8.3 4.1 19.2 Hot flushes Vaginal bleeding Night sweats Nausea Thromboembolic events Vomiting CVA/TIA Other cardiovascular Bone fracture Hypercholesterolemia No arthralgia/joint symptoms or osteoporosis data are available from BIG 1-98 Endometrial cancer shows no significant difference between L and T Adapted from Thürlimann B. St Gallen presentation 2005
ATAC vs BIG 1-98: bone fractures ATAC (A vs T) BIG 1-98 (L vs T ) Patients Patients with bone fracture 340 vs 237 (11.0% vs 7.7%) 1.49, p<0.0001 228 vs 162 (5.8% vs 4.1%) 1.44, p=0.0006 Odds ratio, p value 2.2 vs 1.5 (per 100 patient years) 2.3 vs 1.6 (per 100 patient years) Bone fracture rate Adapted from ATAC Trialists’ Group. Lancet 2005;365:60-62 ; Thürlimann B. St Gallen presentation 2005
ATAC: fracture risk is predictable and manageable 3 Annual rates, %* 2.5 2 1.5 1 Anastrozole 1 mg od Tamoxifen 20 mg od 0.5 0 0 1 2 3 4 5 6 Years since randomisation Number at risk Years Arimidex Tamoxifen 0 3092 3094 1 2923 2932 2 2724 2741 3 2553 2579 4 2393 2401 5 2070 2100 6 845 846 *Calculated using Kaplan-Meier estimates Howell A. SABCS presentation 2004
ATAC vs BIG 1-98: endometrial cancer ATAC (A vs T) BIG 1-98 (L vs T ) Patients Patients with endometrial cancer 5 vs 17 (0.2% vs 0.8%) 0.29, p=0.02 6 vs 15 (0.2% vs 0.4%) 0.40, p=0.078 Odds ratio, p value Adapted from ATAC Trialists’ Group. Lancet 2005;365:60-62 ; Thürlimann B. St Gallen presentation 2005
BIG 1-98: Grade 3-5 cardiovascular events Letrozole(n=3965) Tamoxifen(n=3984) Patients CVA/TIA Thromboembolic Other cardiovascular 46 (1.2%) 30 (0.8%) 143 (3.6%) 42 (1.1%) 79 (2.0%) 101 (2.5%) There is a significantly higher number of other cardiovascular events on letrozole compared with tamoxifen (p=0.006) Thürlimann B. St Gallen presentation 2005
BIG 1-98: death without recurrence Cumulative incidence 20 Proportion failure (%) 5-year difference (L-T) = 1.30.6% p=0.08 (based on CI) 15 Letrozole (L) Tamoxifen (T) 10 3.1% 5 1.4% 1.8% 0 0.8% 0 1 2 3 4 5 Years from randomisation Thürlimann B. St Gallen presentation 2005
BIG 1-98: deaths without recurrence(non-breast cancer deaths) Letrozole(n=4003) Tamoxifen(n=4007) Patients Total CVA thromboembolic cardiac other Overall p value based on cumulative incidence 55 7 3 26 19 38 1 2 13 22 0.08 In ATAC, the numbers of cardiovascular deaths are comparable between anastrozole and tamoxifen (49 vs. 46, respectively) Adapted from Thürlimann B. St Gallen presentation 2005
ATAC: deathsMedian follow-up 68 months Anastrozole(n=3125) Tamoxifen(n=3116) Patients All deaths non-breast cancer deaths cerebrovascular cardiac 411 176 14 49 420 155 21 46 A detailed review found that the non-breast cancer deaths in the anastrozole arm were due to a variety of apparently unrelated causes, with no link to anastrozole ATAC Trialists’ Group. Lancet 2005 ;365:60-62 ATAC Trialists’ Group. Lancet 2005 In Press
Comparison of safety between ATAC and BIG 1-98 Compared with tamoxifen A NS L NS ? ? ? Endometrial cancer Risk of stroke Venous thromboembolic events Cardiovascular deaths Joint symptoms Fractures Hot flushes Vaginal bleeding Vaginal discharge Hysterectomy ? – not reported
ATAC: tolerability and safety summary vs tamoxifen • Compared with tamoxifen, anastrozole is associated with significantly fewer: • SAEs, treatment-related AEs and withdrawals due to SAEs or AEs • potentially life-threatening AEs such as endometrial cancer, thromboembolic and cerebrovascular events • No new safety concerns have emerged with long-term follow-up. There is no issue with cardiovascular safety • Anastrozole now has a known, predictable and manageable safety profile Only anastrozole has a tolerability profile of this robustness and maturity, as it covers more than 5-years’ follow-up AEs = adverse events;SAEs = serious AEs The ATAC Trialists’ Group. Lancet 2005; 365: 60-62; Howell A. Breast Cancer Res Treat 2004; 88 (Suppl 1): S7, abs 1
BIG 1-98: tolerability and safety summary vs tamoxifen • Serious safety concerns about letrozole have emerged in this first analysis • increased incidence of stroke and cardiovascular events • increase in number of cerebrovascular and cardiovascular deaths • No significant reduction in the incidence of endometrial cancer was observed • The long-term safety profile of letrozole is unknown at this stage • cardiovascular effects of letrozole require further evaluation BIG 1-98 has raised serious safety concerns for letrozoleat this early stage
Conclusions (1) • The ATAC completed treatment analysis extends and strengthens the evidence that 5 years of anastrozole is significantly more effective and better tolerated than 5 years of tamoxifen • The efficacy benefit continues to increase with time and extends beyond the completion of therapy • These data support using anastrozole as initial adjuvant therapy The higher rates of recurrence, adverse events, and withdrawals from treatment with tamoxifen and the substantial benefit of anastrozole over the first3 years justify the approach of offering the most effective therapy at the earliest opportunity
Conclusions (2) • BIG 1-98 provides further evidence that tamoxifen should no longer be the standard of care for EBC • No overall efficacy benefits have emerged for letrozole in BIG 1-98 that have not already been demonstrated for anastrozole in the ATAC trial • There appear to be marked differences emerging in the safety of the aromatase inhibitors in the adjuvant setting • women treated with letrozole have a greater risk of stroke and cardiac events • The ATAC completed treatment analysis demonstrates that the overall benefit:risk profile remains clearly and consistently in favour of anastrozole • Only anastrozole has established efficacy and safety with>5 years’ long-term follow-up data