Download
1 / 41
410 likes | 539 Vues
Explore the anatomy, endocrinology, types, and management of pituitary tumors, including surgical approaches and post-operative complications. Learn about the presenting signs, diagnostic imaging, and surgical indications. Increase your knowledge about this complex condition.

E N D
Pituitary Tumors Jerome M. Volk III, HO V LSU Department of Neurosurgery
Anatomy • The pituitary gland weighs 0.6 g. • It is composed of an anterior adenohypophysial component in apposition with a morphologically, embryologically, and functionally distinct posterior neurohypophysial component.
Embryology • Entirely ectodermal in origin • Adenohypophysis • Develops from Rathke’s pouch • Upward invagination • Neurohypophysis • Develops from the infundibulum • Downward extension of the floor of the diencephalon
Endocrinology • Anterior portion (Adenohypophysis) • Follicle stimulating hormone (FSH) • Leutinizing hormone (LH) • Adrenocorticotrophic hormone (ACTH) • Thyroid stimulating hormone (TSH) • Prolactin • Growth hormone (GH)
Endocrinology • Posterior gland (Neurohypophysis) • Oxytocin • Uterine contractions and lactation • Anti-diuretic hormone • SIADH-increased water resorption, low sodium • DI-increased urination, high sodium
Epidemiology • Pituitary tumors account for 10-15% of all primary brain tumors • Highest incidence between the 3rd and 6th decade • More common in women • Genetic predisposition seen only in MEN-1. • Although this accounts for only 3% of pituitary tumors
Sellar masses: • Tumors • Adenohypophysial origin • Pituitary adenoma (macro and micro) • Pituitary carcinoma • Neurohypophysial origin • Granular cell tumor • Nonpituitary origin • Meningioma • Glioma • Craniopharyngioma • Germ cell tumor
Sellar masses: • Cysts and Hamartomas: Epidermoid, arachnoid, rathke cleft, dermoid, hypothalamic hamartoma • Metastatic: carcinoma, lymphoma • Infammatory: sarcoidosis, langerhans cell histiocytosis, lymphocytic hypophysitis • Vascular: aneurysm, cavernoma
Pituitary Adenoma • Classified by: • Endocrine/Clinical • Pathology • Imaging
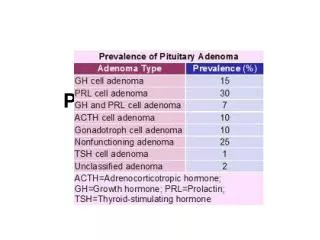
Pituitary Adenoma • Prolactinoma: • 30% of pituitary adenomas • More commonly micradenomas • Present as amenorrhea with galactorrhea • Prolactin levels > 200 ng/ml (if less worry about stalk effect) • First line treatment is pharmacologic • Dopamine agonists (bromocriptine
Growth Hormone Secreting Tumor • Most commonly macroadenoma • Occur in the 4th and 5th decade • Coarse facial features, thickening of lips, enlargement of nose • GH level > 5 ng/ml • Initial treatment is surgery
Corticotroph Secreting Adenomas • 8-10% of pituitary tumors • Cushing’s Disease • Hypercortisolemic state generated in response to an ACTH-secreting pituitary tumor. • Weight gain, truncal obesity, buffalo hump • Free cortisol level • no cortisol suppression on low-dose dexamethasone testing, cortisol suppression on high-dose dexamethasone testing, and moderately elevated ACTH levels • Surgery is best option
Thyrotroph adenomas • Less than 1% of pituitary adenomas • Manifest with signs of hyperthyroidism • High TSH with high Free T4 • Surgery is first option • Clinically silent • 1/4th of pituitary tumors • Surgery is first option
Presenting signs and symptoms: • Pituitary hyperfunction • Pituitary insufficiency • Mass effect • Headache-pressure on V1 at diagphragma sella • Loss of vision-compression of optic chiasm • Hydrocephalus-compression on third ventricle • Hypothalamic abnormality-sleep, alertness, emotion
Labs and images • Imaging: • MRI brain with and without IV contrast (include thing cuts through pituitary) • Tumor enhances less than gland • Labs: • Prolactin, FSH, LH, GH, ACTH, testosterone, GH, cortisol, IGF-1 • Visual Fields: • To be performed by an ophthomalogist
Surgical indications: • Progressive mass effect • Worsening of vision • Failure of prior treatment • Pharmacologic • Prolactinoma • Cushing’s disease • Radiation
Surgical indications: • Pituitary Apoplexy • The abrupt and occasionally catastrophic acute hemorrhagic infarction of a pituitary adenoma • Present with acute headache, meningismus, visual impairment, ophthalmoplegia, and alteration in consciousness • Glucocorticoid replacement is the most important first step due to adrenal insufficiency • Followed by urgent surgical decompression
Surgical Approaches: • Transsphenoidal • Endoscopic • Endonasal • Sublabial transseptal • Transcranial • Pterional • Subfrontal
Transsphenoidal Endonasal Sublabial
Post-operative Complications: • Diabetes Insipidus • Follow urine output and Sodium levels • CSF leak • Check for rhinorrhea • Hemorrhage/Apoplexy • Worsening vision