PUBH 6165 (WEEK 7) Application
PUBH 6165 (WEEK 7) Application. Instructor: Dr Jalal Ghaemgham Project: Malaria Date: July 31, 2009 School: Walden University Student: Kenneth Odimgbe. The audience. This presentation is geared towards a group of health care practitioners at a local hospital in Atlanta , Georgia, U.S.A.

PUBH 6165 (WEEK 7) Application
E N D
Presentation Transcript
PUBH 6165 (WEEK 7) Application Instructor: Dr JalalGhaemgham Project: Malaria Date: July 31, 2009 School: Walden University Student: Kenneth Odimgbe
The audience • This presentation is geared towards a group of health care practitioners at a local hospital in Atlanta , Georgia, U.S.A. • They are , Nurses, Allied health practitioners, Nursing Assistants and Hospital environmental workers. • As part of this audience and as a survivor, I was asked as a volunteer to give a first hand testimony of my experience with malaria. • Use that experience to clarify some issues and help any of the hospital employees in case they find themselves in a familiar situation.
Reasons for presentation • In a few days , this Medical team will be travelling to Haiti (A tropical climate country with history of malaria) on a medical mission for two weeks. • Although they have medical backgrounds, their knowledge and experience with malaria is very limited. • Malaria is not common here in the United States and as such, they are not familiar with it. • To create a better understanding between these healthcare workers and their potential patients who might have been infected with malaria.
Other Reasons for this presentation • To create better understanding of malaria in a group of individuals not familiar with the disease. • Although this topic might be very basic and elementary, it could broaden the knowledge of what was already known before the presentation. • After this presentation, the practice of placing malaria patients in hospital isolation rooms with masks and gowns might not be necessary unless the Doctors came up with other diagnosis to prove otherwise.
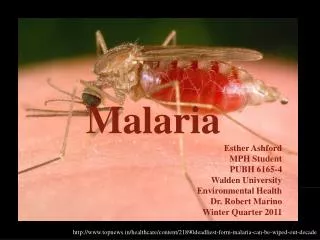
Description of Malaria • A vector- borne infectious disease caused by protozoan parasites that infects a certain type of mosquito which feeds on humans. These mosquito parasites are classified into four classes: plasmoduimfalciparum, Plasmodium vivax, plasmoduimOvale, and plasmoduim malaria. Malaria is one of the most common infectious diseases and an enormous public health problem (CDC). • Most dangerous among them is P. Falciparum because if not treated promptly, may lead to death ( CDC).
How do we get Malaria • When bitten by a female Anopheles mosquito that was infected through a previous blood meal taken on an infected person. • A mosquito bites an infected person, takes a small amount of blood that contains a microscopic malaria parasites( CDC). • In a weeks time, with the next blood meal, the parasites mix with the mosquito,s saliva and are injected into the person being bitten (CDC, 2008). • An incubation period of 7-30 days could be a time frame for malaria before it manifests (Jayashree , 2007)
Other forms of Malaria transmission • Shared syringes or needles contaminated with malaria parasites . Might be common in Haiti . • From Mother to unborn infant before or during delivery (Congenital Malaria). • These forms of transmission is possible because the malaria parasite is found in red blood cells (CDC, 2008).
Is Malaria Contageous ? • No • Malaria is not spread from person to person like cold or the flu. • Some of the patients that will come in contact with the medical team in Haiti might have had malaria. Basic precautions are all that is needed. • Do not worry, there is no infection from casual contact with them.
Location of Malaria • Very widespread in tropical regions of Africa, subtropical regions of America , Asia and Middle east (Davis & Shiel, 2009). • Sub –Sahara Africa has about 90% of World,s malaria. • Asia : mostly in India,Parkistan, Bangladesh, Thailand, Vietnam,Laos,Myanmar, Indonesia. • South America: mostly in Brazil,Peru,Colombia, Bolivia,Ecuador, venezuela. • Central America and South Mexico: mostly in Honduras, Nicaragua and Guatemalia. • Europe: mostly in Turkey,Armenia, and Arzebaijan.
Susceptibility to Malaria • Mostly Individuals that live in countries with malaria as described above. • Travelling to countries with malaria e.g Haiti where the medical mission will take place. • From mother to Child during delivery. • Through blood transfusion (very rare).
Individuals mostly at risk of getting sick and dying of malaria • Individuals exposed to P. Falciparum • Individuals with little or no immunity to malaria e.gtravellers from areas with no malaria like our medical team about to go on medical mission, Pregnant women, young children (between the ages of 1-5 yrs). • Lack of knowledge about the disease due to living arrangements or living in rural areas. A lot of the patient population the medical team will serve in Haiti are under this category. • Lack of financial ability to get medication. • Lack of access to health insurance.
How to acquire malaria immunity • By being born and living in a malaria risk country e.g Haiti or any tropical country where malaria is already endemic. • Previous exposure to malaria parasites. • Prior visit to a travel clinic and getting preventive medications against mosquito bites (CDC) before any travel to malaria endemic areas like the place we will be heading to in few weeks.
Diagnosis of malaria • By microscopic blood exam. First visualized by Charles Laveran in 1880.A Giemsa stain is used to stain the specimen thereby giving the parasite a distinctive appearance (Davis & Shiel, 2009) . It is still the gold standard for diagnosis. • Alternatively, urine and saliva could be used as they are less invasive specimens. • Use of thin and thick films to make definitive diagnosis. • Use of Malaria rapid diagnostic test whereby in 15-20 mins, a finger stick or venous blood is tested. No lab is needed here. • Optimal-IT tests. • Paracheck PF test. • Molecular methods. • Serology: detects antibodies against malaria parasite by using immunofluorescence(IFA) or Enzyme linked immunosorbent assay(ELISA).Serology does not detect current infection but rather measures past expirience.
Signs and symptoms of malaria • Flu like symptoms and fever. • Headache and convulsions. • Muscle aches and joint pain. • Tiredness. • Diahrrea and vomiting. • Anemia (due to hemolysis). • Jaundice(yellow coloring of eye and skin) due to the loss of red blood cells.
Consequencies of not treating malaria • May lead to seizures. • Kidney fairlure. • Mental confusion. • Coma. • Possibly death. Mostly noticed in the P. falcipraum type.
Preventing malaria during the medical Mission in Haiti • Keep away from mosquito bite especially at night. • Kill the parasites by taking antimalarial medications prescribed by the Doctor. • Before leaving for the Medical mission, prophylactic or preventive meds should be administered (4-6 weeks). • If going outdoors at night, wear long sleeved clothes. • Use of insect repellents in the house should be encouraged. • Use of bed nets that is treated with insecticide. • Spray home walls with insecticides in order to kill adult mosquito found inside the house (WHO).
Levels of prevention when in Haiti on Medical Mission • Please avoid bites by parasite carrying mosquitoes. • Before travel, see your Physician, a tropical disease specialist or visit a travel health Clinic 4-6 weeks in order to obtain the necessary prophylaxis(preventive) meds that stops malaria parasites development in the blood.
Current prophylactic medications • Mefloquine (Lariam) • Chloroquine • Proquanil • Pyrimethamine (daraprim) • Doxycycline • Hydroxichloroquine (paquenil)(FDA).
Vaccines for Malaria • Type 1 vaccine : The SP1666, was developed by Manuel Elkin Patarroyo in 1987. Had a 75% efficacy rate. First used in Tanzania, then Gambia, then the CSP, followed by the R32LR. • Mostly for those exposed to P. falciparum malaria in the sub –Saharan Africa. The main objective here is to reduce the number of severe malaria cases and deaths in infants and children exposed to high transmission rates (CDC). • Type 2 vaccine: Also called travellers vaccine. It aims to prevent all cases of clinical symptoms in patients with no past exposure history (CDC). • The most successful vaccine so far is the RTS,S/AS02A, has been used in Gambia (Good & kemp ,2004).
Immune responses elicited by parasite • Two main types: • Anti-Parasitic Immunity: Has an antibody response and a cell- mediated immune respone. Both ensures maximum chance of preventing disease( Saul, 2004) . • Anti toxic Immunity: Responses to address the symptoms like respiratory distress and cerebral symptoms (Hill, 2004) .
Treatment of Malaria • (In endemic areas), treatment needs to be initiated within 24 hours after the first symptoms. • Uncomplicated malaria can be treated on an ambulatory basis ie without hospitalization. • Severe malaria should be hospitalized immedietly. • (In non endemic areas), patients with uncomplicated or severe malaria should be kept under clinical observation if possible (WHO) .
Standard Medications for Malaria Treatment • Quinine/ quinidine • Mefloquine (Lariam) • Fansidar (Sulfadoxine-pyrimethamine) • Chloroquine • Doxycycline • Atovaquone-Proguanil ( Malarone) • Artemisin derivatives -mostly found overseas, not licensed in the United States. • Primaquine- administered for dormant parasite liver forms(hypnozites) and prevents relapses. • Amodiaquine • Lumefantrine
Side effects of Malaria Medications • Please check with your physician about allergic response before taking malaria medication. • Continous body irritation and scratching can occur with administration of chloroquine. • Other adverse effects like nausea, diahrrea, Sunburn, vivid dreams, vision disturbances, hallucination could be observed as adverse effects with malaria medications. • However, with meals these advers effects could be less pronounced.
Malaria in sub-Sahara Africa • 1 million people die of malaria in the world, 90% of them are in Africa, most of them are young and this translates to approximately 30 second a child is dead (WHO). • Since 2000, april 25th has was declared Africa Malaria day. • 44 African heads of states and representatives met and signed a declaration in Abuja,Nigeria. • Their countries were committed to halve malaria deaths by 2010 in Africa (CDC). • CDC, nearly after 60 years of it,s creation to fight malaria in the US participates actively in this Worldwide battle especially in endemic areas of Africa. • Since 2004, the CDC has joined in the global observation of Africa malaria day by launching a new website https://www.cdc.gov/malaria/spotlights/index_042304.htm
Conclusion • As healthcare professionals that will soon be on a medical mission overseas, it is essential that we make use of these elementary informations. • They are very basic and please consult your private Physician for more information and guidance. • These steps outlined in the presentation will help in addition to what you already know about malaria. • Please , do not buy medications in the streets when abroad because it comes with risks even though they may be cheaper and could be poorly produced. • Wish all safe journey to haiti as we continue to render charity work to those who otherwise might not be able to afford medical care.
Further reading • Malaria is a very vast topic and more information can be found in: • www.Cdc.gov/malaria/faq/htm. • www.Pubmedcentral.nih.gov • www.answers.com/topic/malaria • www.malaria.com • www.malaria.org • www.medicinet.com/malaria • www.african-safari-journals.com/malaria-tablets.html • www.cdc.gov/travel/malariadrugs.htm
References • CDC (2004). Globanization of malaria. Retrieved on July 17, 2009 from https://www.cdc.gov/malaria/spotlights/index_042304.htm. • CDC (2008). Malaria Transmission. Retrieved on July 18, 2009 from http://www.cdc.gov/malaria/article.htm. • Davis, C., Shiel, W. (2009) Locating Malaria. Retrieved on July 18, from https://www.medicinenet.com/malaria/article.htm. • Good, M., Kemp, D. (2004) Overview of Vaccine strategies for malaria and New generation Vaccines, 3rd edition. • Hill, C (2004) Malaria vaccine developments. The Lancet. 363: 150-156 • Jayashree, P . ( 2007) Malaria symptoms, Cause & treatment. Retrieved on July 15, 2009 from http://www.buzzle.com/articles/malaria-disease-symptoms-causes-treatment.html. • WHO (2008). Facts on Malaria. Retrieved on July 18, 2009 from https://www.who.int/topics/malaria/en