Antiinfection immunity
310 likes | 518 Vues
Antiinfection immunity. Relationship between host and microorganism microorganisms - commensal - potential pathogens - pathogenic microorganisms

Antiinfection immunity
E N D
Presentation Transcript
Relationship between host and microorganismmicroorganisms - commensal - potential pathogens - pathogenic microorganisms - microorganisms can cause damage to the body by direct mechanisms (toxins, cytopathic effect), or indirect, which initiate harmful immune reactions In defense against various microorganisms are, despite a predominant type of immune response, involved all elements of nonspecific and specific immunity.
Use of receptors on host cells as a gateway of infection CD4 - HIV, herpesvirus7 CD21 (CR2) - EBV CD71 - hepatitis B virus CD81 - hepatitis C virus b1 integrins - Yersinia, pathogenic E. coli b3 integrins - Borrelia
Mechanisms of microorganisms escape before defense system - conceal the cells, integration into the genome and the persistence in the latent form (herpes viruses, retroviruses) - variability of surface molecules (influenza, HIV ...) - suppression of MHC gp expression in infected cells (adenoviruses, herpes viruses) - suppression of Ag presentation (blocking cleavage antigen)
- suppression of inflammatory response by production of virus analogues of cytokines or their inhibitors - inhibition of complement by production of protective proteins (herpes), secretion of proteases, which inactivate C3a and C5a, cell wall protects against membranolytic effect of complement - cleavage of blocking sIgA antibodies - the use of cytokines produced by the host to create an optimal environment (TNF stimulates HIV replication)
- integration of the host's own molecules into the microbial wall (borrelia burgdorferi) - antigenic mimicry - surface structure mimic the structure of the host organism cells - inhibition of phagocytosis, inhibition of fusion phagosome with lysosomes; escape from phagosome to the cytoplasm, inhibition of acid pH inside phagolysosome - production of antagonistic peptides (hepatitis B virus, HIV)
Defense against extracellular bacteria -gram-negative, gram-positive cocci, bacilli - for their elimination is necessary opsonization (C3b, lectins, antibodies ...) - neutrophilic granulocytes are chemotactic attracting to the site of the infection (C5a, C3a and chemotactic products of bacteria) - absorbed bacteria are destroyed by the microbicidal systems (products NADP-H oxidase, hydrolytic enzymes and bactericidal substances in lysosomes) - phagocytes production of proinflammatory cytokines (IL-1, IL-6, TNF) that induce an increase in temperature, metabolic response of the organism and synthesis of acute phase proteins
- in later stages of infection are stimulated antigen-specific mechanisms - plasma cells initially produce IgM isotype after isotype switching produce IgG1 and IgA (opsonization) - sIgA protect against intestinal and respiratory infections by bacteria - bacteria with a polysaccharide capsule may cause T-independent IgM antibody production (after the establishment to the bacteria activate the classical complement path) - after infection persist IgG, IgA (protective effect), and memory T and B lymphocytes
- in the defense against bacterial toxins apply neutralizing antibodies (Clostridium tetani and botulinum ...) - "indirect toxins - bacterial Lipopolysaccharide (LPS) stimulates big number of monocytes to release TNF, which can cause septic shock - extracellular bacterial infections are especially at risk individuals with disorders in thefunction of phagocytes, complement and antibody production
Defense against intracellular bacteria and molds - intracellular parasitism is given by the ability of microorganisms to escape microbicidal mechanisms of phagocytes - mycobacteria, some yeasts and molds - macrophages, which absorbed them, produce IL-12 → TH1 differentiation, production of IFNg and membrane TNF → activation of macrophages and induction of iNOS - plasma cells under the influence of IFNg produce IgG2, immune complexes containing IgG2 bind to Fc receptors on macrophages and thus stimulate - in the defense against intracelular parasites, which escape from phagolysosomes apply TC lymphocytes - intracellular microorganisms infections are at risk individuals with certain disorders of phagocytes and defects of T lymphocytes
Defense against viruses- interferons - in infected cells is induced production of IFNa and IFNb (prevents viral replication and in uninfected cells cause the anti-virus status); IFNg stimulates the conversion to activated macrophages (iNOS) - NK cells - ADCC (Antibody-dependent cell-mediated cytotoxicity) = cytotoxic reaction depends on the antibodies; the NK-lymphocyte recognizes cell opsonized with IgG by stimulation Fc receptor CD16 and then activate cytotoxic mechanisms (degranulation) - infected macrophages produce IL-12 (a strong activator of NK cells) - in the defense against cytopathic viruses mostly applied antibodies: - sIgA inhibit mucosal adhesion of viruses (defense against respiratory viruses and enteroviruses) - neutralizing IgG and IgM antibodies activate the classical way of complement, which is capable of some viruses lysis - IgA and IgG derived in viral infection have a preventive effect in secondary infection
- effector TC lymphocytes destroy infected cells in direct contact (granzym/perforin; FasL) and by produced cytokines (lymfotoxin) - some viruses after infection integrate into the host genome, where persist for years (varicella zoster, EBV, papillomavirus) - by these infections are at risk individuals with T lymphocyte immunodeficiency and with combined immune disorders - increased susceptibility to herpes infections in individuals with dysfunction of NK cells.
Defense against protozoa parasites - defense against protozoa parasites is similar to bacteria - extracellular parasites - antibodies - intracellular parasites - TH1 lymphocytes and activated macrophages
Defense against multicelular parasites - contact of mast cells, basophils and eosinophils with parasite antigens - TH2 stimulation under the influence of IL-4 (mast cells and other APC stimulated by parasite) - TH2 stimulate B cells with BCR-specific parasite antigens - isotype switching under the influence of IL-4 in IgE - IgE bind to FceRI on mast cells and basophils (antigen-specific receptors) - establish of multivalent antigen (multicellular parasite) using the IgE to highafinity Fc receptor for IgE (FcRI)
- aggregation of several molecules FcRI - initiate mast cell degranulation (cytoplasmic granules mergers with the surface membrane and release their contents) - activation of arachidonic acid metabolism (leukotriene C4, prostaglandin PGD2) - amplification of inflammatory responses - start of production of cytokines (TNF, TGF, IL-4, 5,6 ...) by mast - in later stages are activated TH1 and are produced antibodies of other classes - eosinophils fagocyte complexes of parasitic particles with IgE via their receptors for IgE - eosinophils use against parasites extracellular bactericidal substances released from granules (eosinophil cationic protein, protease)
Possibilities of the therapeutic effect on the immune system
Causal treatmenta)stem cell transplantation - for serious congenital disorders of the immune system (some lymphoproliferative and myeloproliferative disorders) - complications: infectious complications Graft-versus-host - obtaining stem cells - the collection from shovel hip bone - from umbilical cord blood - from peripheral blood after stimulation with GM-CSF
b)gene therapy - with a suitable expression vector is introduced functional gene (to replace dysfunctional gen) into the lymphocytes or stem cells - used as a treatment for some cases of SCID
Substitution treatment - autologous stem cell transplantation following chemotherapy and radiotherapy - treatment with intravenous immunoglobulin (derived from plasma of blood donors) - substitution of C1 inhibitor for hereditary angioedema - substitution of erythropoietin in patients with chronic renal failure - substitution of G-CSF in agranulocytosis
Non-specific immunomodulation therapyImmunomodulation = medical procedure to adjust the disrupted immune function a)non-specific immunosuppressive therapynonspecific = affects not only autoreactive and aloreactive lymphocytes, but also other components of immunity (risk of reduction antiinfectious and anti-tumor immunity) - used for treatment of autoimmune diseases, severe allergic conditions and for organ transplantation
corticosteroids - anti-inflammatory, immunosuppressive effects - blocking the activity of transcription factors (AP-1, NFkB) - suppress the expression of genes (IL-2, IL-1, phospholipase A, MHCgpII, adhesion molecules) - inhibition of histamine release from basophil - higher concentrations induce apoptosis immunosuppressants affecting the metabolism of DNA - cyclophosphamide - methotrexate immunosuppressant selectively inhibiting T lymphocyte - cyclosporin A (inhibits the expression of IL-2 and IL-2R in activated T lymphocytes) - monoclonal antibody anti-CD3 (immunosuppression after transplantation, treatment of rejection crises)
b)anti-inflammatory and antiallergic treatmentnonsteroidal anti-inflammatory drugs antihistamines - blocking H1 receptor - reduce the expression of adhesion molecules - reduce the secretion of histamine ... inhibitors of inflammatory cytokine - receptor antagonist for IL-1 - monoclonal antibodies against TNF - thalidomide (TNF inhibitor)
c) non-specific immunostimulant therapyimunostimulancia - stimulate the immune system synthetic immunomodulators - Methisoprinol (Isoprinosine) - used in viral infections with more severe or relapsing course bacterial extracts and lysates - Broncho-Vaxom - prevention of recurrent respiratory tract infections- Ribomunylproducts of the immune system - IL-2 - renal adenocarcinoma - IFNa, IFNb - viral hepatitis, some leukemia - Erythropoietin- G-CSF, GM-CSF - neutropenia
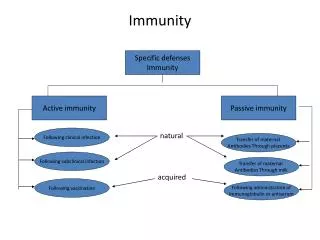
Antigen-specific immunomodulatory therapy specific immunomodulation = induce an immune response or tolerance against a specific antigen a) active immunization = use of antigen to induce an immune response that can later protect against a pathogen bearing the antigen (or antigen like him) - immunization vaccines made from inactivated or attenuated microorganisms or their antigens (polysaccharide capsule, toxins) - creates long-term immunity - activate cellular and antibody immunity - administration of antigen injectable, oral - prophylaxis - risk of causing infection or anaphylactic reactions
Active immunization DTP (diphtheria, tetanus, Pertussis) Haemophilus influenzae Neisseria meningitidis Pneumococci BCG (Bacillus Calmette-Guérin) MMR (measles, mumps, rubella) Poliomyelitis Hepatitis A, B • experimentally implementing specific vaccination against cancer
b) passive immunization- natural - transfer of maternal antibodies in fetal blood - therapeutically - the use of animal antibodies against various toxins (snake toxins, tetanus toxin, botulinum toxin) - prophylaxis - the human immunoglobulin from immunized individuals (hepatitis A, rabies, tetanus) - Anti-RhD antibodies - preventing maternal immunization with RhD+ fetus - provides a temporary (3 weeks) specific humoral immunity - the risk of inducing anaphylactic reactions
c) specific immunosuppression= induction of tolerance against a specific antigen the clinical studies: - induction of tolerance by oral administration of antigen - allergen immunotherapy (pollen, insect poisons)