Download
1 / 24
240 likes | 474 Vues
Comparison of intrathecal isobaric bupivacaine-morphine and ropivacaine-morphine for CS delivery Department of Anaesthesiology and Intensive Care and Department of OB&GYN, Facultry of medicine,Selcuk University,Konya,Turkey. BJA 90(5):659-64(2003). BACKGROUND. Ropivacaine A new long acting

E N D
Comparison of intrathecal isobaric bupivacaine-morphine and ropivacaine-morphine for CS delivery • Department of Anaesthesiology and Intensive Care and Department of OB&GYN, Facultry of medicine,Selcuk University,Konya,Turkey. • BJA 90(5):659-64(2003)
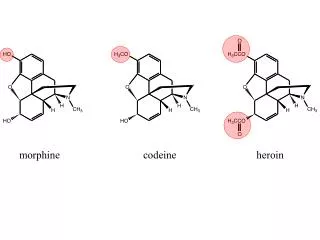
BACKGROUND • Ropivacaine • A new long acting • Amide • A high pKa and low lipid solubility • Block sensory N.> motor N. • Less cardiotoxic than bupivacaine in vitro • Higher threshold for CNS toxicity than racemic bupivacaine
BACKGROUND • In previous study • Intrathecal hyperbaric ropivacaine :- non OB Sx. Or labour analgesia combined with sufentanyl or fentanyl (Chung and colleagues) • A dose-response study with isobaric ropivacaine in C/S (Khaw and colleagues)
OBJECTIVES • Prospective, double-blind, randomized study • Compare the analgesia and spinal block characteristics of 0.5% isobaric ropivacaine+morphine and 0.5% isobaric bupivacaine+morphine in C/S
MATERIALS AND METHODS • ??????? 50 ASA I or II + elective CS of single babies at term • Exclusion :-cardiac disease , haematological dis., DM, eclampsia, bleeding or coagulopathy, fetal distress or known fetal anomalies • Premed. :- sodium citrate 30 ml 30 min before • Fluid loading :- 6% hydroxyethystarch 10 ml/kg
MATERIALS AND METHODS • A computer-generated randomization table group RM ( n=25 ) and group BM ( n=25 ) • RM (n=25 ) 0.5% isobaric R. 15 mg + MO 150 ug • BM (n=25 ) 0.5% isobaric B. 15 mg + MO 150 ug • Anaesthetist not involved the data • The investigator were blinded
MATERIALS AND METHODS • Monitors :- HR, MAP, SpO2, RR, • IV MT;- LRS 10 ml/kg/hr during surgery • Spinal anaesthesia • Sitting position • Quincke needle NO.25 • L3-4 or L4-5 • Study solution 3.7 ml administered 30 s(0.12 ml/sec) • Confirmed by aspiration and re-injection of 0.2-0.3 ml CSF before and after • Turned to supine with left uterine displacement position
MATERIALS AND METHODS • After the spinal block:- HR,RR,SpO2 and MAP q 1 min until delivery and then q 2 min. • Hypotension = 20% of baseline MAP • Rx. Hypotension with ephredine 5-10 mg and total ephredine were recorded • Supplement O2 with facemask
MATERIALS AND METHODS • Sensory block loss of pin-prick sens. (20 G hypodermic needle) at MCL q 5 min until reached T5 dermatome the q 10 min • Motor block Bromage scale(0=no motor block,3=complete block of lower ext) q 1 min until complete block q 30 min • The motor block when the sensory level reached T5 were recorded
MATERIALS AND METHODS • The time from skin incision to delivery • After delivery,umbilical blood gas • APGAR scores at 1 and 5 min • Side effect and sedation or GA • Maternal sedation scores • 48 hrs. After surgery :- prutitus,headache,backache,resp.distress,N/V • The quality of anaesthesia (by anaesthetists),the quality of MR (by surgeon)
STATISTICAL ANALYSIS • SD of time to recovery from motor block and time to regression of two segment wiht ropivacaine power analysis • 30-min difference in mean duration of motor block or a 10- min difference in mean duration two segment regression between 2 groups two-side alpha of 5% and beta of 20% • Group size of 16-17 was necessary • One-way and two-way ANOVA repeated measures
STATISTICAL ANALYSIS • Unpaired and paired t-tests for quantitative • X2 test for categorical data • P < 0.05 was significant
RESULTS • As table
DISCUSSION • Similar sensory block and PO analgesia,shorter duration of motor block,less ephredine requirement,similar APGAR scores and umbilical pH and similar SE • An equal dose of R. And B. (15 mg) and ropivacaine dose ~ ED50(Khaw and coll.) • Prolong PO analgesia after CS RM is considered to be less potent than BM But similar two-segment regression(Chung and coll.)
DISCUSSION • The equipotent ratio between B. And R. Is 3:2 or 2:1 R. Expected to lead to less cephalad spread than similar B. Dose( Parlow and coll. demon.that adding opioid alter the density and spread in CSF) • Pharmacodynamic studies not know why RM=BM Further studies
DISCUSSION • Previous study:-Motor block of BM > RM but dose is 3:2 but in this study dose is 1:1 • PO neurological symptoms • Hypotension
THANK YOU • FOR YOUR ATTENTION • P.Chatchawarat,MD
Can you find this information in the paper? • What is the research question? • What is the study type? • What are the outcome factors and how are they measured? • What are the study factors and how are the measured? • What important potential confounders are considered?
Can you find this information in the paper? • What are the sampling frame and sampling method? • In an experimental study how were the subjects assigned to groups? In a longitudinal study how many reached final follow up? In case-control study are the controls appropriate?
Can you find this information in the paper? • Are statistical tests considered? • Are the results clinically/socially significant? • What conclusions didthe authors reach about the study question?