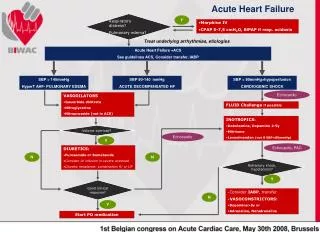
Acute Heart Failure
Acute Heart Failure. Approach to the Patient in The Emergency Room Gad Cotter MD. Disclosure: Grants from Actelion , Novacardia , Merck, Cytokinetics /Amgen, Cardio3, Bioheart, Nile thera, Corthera, Bioheart, Novartis, Travena, NIH. …The Reality. Higher than COPERNICUS Almost at REMACH….

Acute Heart Failure
E N D
Presentation Transcript
Acute Heart Failure Approach to the Patient in The Emergency Room Gad Cotter MD. Disclosure: Grants from Actelion , Novacardia , Merck, Cytokinetics /Amgen, Cardio3, Bioheart, Nile thera, Corthera, Bioheart, Novartis, Travena, NIH.
…The Reality Higher than COPERNICUS Almost at REMACH… Lee DS, Am. J. Med. 2004
So what is it about???? Classification By Syndrome
Classification to specific Syndromes • Acute Heart Failure (Suggested new name: Acute vascular failure - AVF): Rapidly evolving pulmonary congestion + blood pressure • rapid respiratory failure, multi-organ failure and death. (Elderly, female, preserved EF, mild chronic CHF) • Acute Decompensated Heart Failure - ADHF: Slow deterioration in severe chronic heart failure, • slowly progressive low cardiovascular perfusion and pulmonary congestion, accompanied by relatively blood pressure, peripheral edema and weight gain. (Younger, male, low EF, significant background CHF) • Other: Acute coronary syndromes, arrhythmias (mostly A.Fib), High output failure, RV Failure.
How do we tell them apart ? Acute Vascular Failure Acute Cardiac Failure • Congestion (Chest X-Ray) +++ ++ • Background Chronic HF 0 / + +++ • High BP at admission +++ 0/+ • Low CVS perfusion + +++ • Reduced EF (echo) + +++ • Weight / Leg edema + +++ • Neurohormonal/Inflammatory Activation +++ ++ • Causal factor (Infection) +++ + M. Metra (Brescia) European Working Group on AHF
Acute “Cardiac” Heart Failure • The “core mechanism” is a deterioration in cardiac contractility (“Cardiac Power”) caused by either acute processes (Ischemia, Arrhythmia) or slow processes (LV remodeling and progressive myocardial cell loss).
Acute (Cardiac) Heart Failure Decreasing Cardiac Contractility (Cpo) Inflammatory/ Neurohormonal Activation “Low CVS perfusion” Forward Failure (Effective Blood Volume ) Over Diuresis Arterial Resistance/ Stiffness Renal Impairment / Fluid Accumulation (3-4 Kg) Wedge Compliance Diastolic Dysfunction Central Fluid Redistribution Pulmonary Congestion
What is Cardiac Power? • Cardiac Power is the measure of left ventricular systolic contractility power and is calculated by incorporating flow and pressure domains of the CV system; Hence: Cardiac Power Output = Cardiac Output * Mean Arterial Blood Pressure Cpo = MAP * CO
What is the Range of Cpo? • Cotter, Tan et.al. Curr. Opinion. Card 2003
Cardiac power for the diagnosis of Acute hemodynamic instability instability Cotter, Tan et al. Curr Opin Cardiol 2003, 18:215–222
Predicting Recurrent HF and Death: Cotter, Tan et al. Curr Opin Cardiol 2003, 18:215–222
Acute “Vascualr” Heart Failure • The “core mechanism” is an abrupt increase in vascular stiffness/resistance, probably secondary to neurohormonal/inflammatory excessive activation in response to “normal” insults such as minor infections.
Acute (Vascular) Heart Failure “small Tn Release” Low Cardiac Contractility Reserve (Cpo) Inflammatory/ Neurohormonal Activation “Low CVS perfusion” Forward Failure (Effective Blood Volume ) Over Diuresis Arterial Resistance/ Stiffness Renal Impairment / Fluid Accumulation (0-2 Kg) Wedge Pulmonary Congestion Diastolic Dysfunction Central Fluid Redistribution
First admission Systolic BP in patients admitted for AHF in a “real life” community center Cotter et al. European Journal of Heart Failure 9 (2007) 178–183
Inflammation and Neurohormonal Activation in AHF:Cause for Arterial Stiffness/Vascular resistance, Decreased Contractility and Diastolic Dysfunction? – ET-1 and IL-6 levels in patients admitted with AHF at baseline (0), 2 and 60 days follow-up. Milo, Cotter, et. al. Am. J. Cardiol. 2003
Measuring circulatory and Respiratory Failure Low Cardiac Contractility Reserve (Cpo) Inflammatory/ Neurohormonal Activation “Low CVS perfusion” Forward Failure (Effective Blood Volume ) Arterial Resistance/ Stiffness Renal Impairment / Pulmonary Congestion Central Fluid Redistribution
Severity of congestion = Admission SO2 Recurrent HF/Death Death
Circulatory failure = Admission Sys BP Recurrent HF/Death Death
Combined circulatory and respiratory failure = Admission Sys BP and SO2 Recurrent HF/Death Death
Combined SEVRE circulatory and respiratory failure = Admission Need for pressors or mechanical ventilation Recurrent HF/Death Death
Laboratory Evaluation Low Cardiac Contractility Reserve (Cpo) Inflammatory/ Neurohormonal Activation “Low CVS perfusion” Forward Failure (Effective Blood Volume ) Arterial Resistance/ Stiffness Renal Impairment / Pulmonary Congestion Central Fluid Redistribution
Simple way to measure neurohormoanl activation - Na+ and Glucose Cotter et al JCF 2006
Simple way to measure inflammatory activation – Lymphocyte ratio of WBC differential • Cardiology 2010 in Print
Other Lab Predictors at admission • Troponin? • BNP ? • Endothelin ? • Others ?
Baseline Model Predicting Time to Death Adding Troponin Levels
Baseline Model Predicting Time to Death or Re-hospitalization Adding Troponin Levels
Echo - Changes in Ejection Fraction During Recovery from Pulmonary Edema 0.80 0.60 LV Ejection Fraction During Acute Pulmonary Edema 0.40 0.20 0.00 0.00 0.20 0.40 0.60 0.80 LV Ejection Fraction After Treatment Ghandi et al, NEJM 2001
Echocardiographic Changes During Recovery from Pulmonary Edema • Measures of dyastolic dysfunction improved during follow up: E/A ratio (1.3±0.8 to 1.5 ± 1.0) and E-wave declaration (174 ± 62 to 194 ± 62). • The authors concluded that: “... high BP related wedge pressure increase caused diastolic dysfunction in these patients … and …no changes in EF occurred during the acute heart failure episode”. • Choen-Solal et al in a study of patients with AHF: “…LVEF was poorly predictive while the predischarge Doppler mitral pattern was strongly associated with death or re-admission..” Ghandi et al, NEJM 2001, Choen-Solal et al JACC 2004
Conclusions • ONCE AHF IS DIAGNOSED - Evaluation in the ER should include: • Variables related to respiratory and circulatory failure – mostly oxygen saturation and BP • Lab – Sodium, glucose, kidney function , WBC count with diferencial and possibly BNP and troponin • Echocardiography – to rule out mechanical complications, PE, possibly to evaluate severity of diastolic dysfunction