Association of Type 2 Diabetes with Cognitive Performance in HIV-Infected Patients
This study investigates the relationship between Type 2 diabetes and cognitive function in HIV-infected patients within the ANRS-CO3 Aquitaine cohort. The research emphasizes the higher prevalence of vascular risk factors, such as hypercholesterolemia and diabetes, among this population and their potential impact on cognitive decline. A total of 400 patients were recruited, with 288 undergoing a two-year follow-up, assessing various cognitive domains. Our findings suggest that diabetes and impaired glycemia are associated with lower cognitive performances, underscoring the need for targeted interventions.

Association of Type 2 Diabetes with Cognitive Performance in HIV-Infected Patients
E N D
Presentation Transcript
Carole Dufouil(1,2), Laura Richert (1,2), Mathias Bruyand(1,3), Hélène Amieva (1,2), Frédéric-Antoine Dauchy (3), Carine Greib (4), Jean-François Dartigues (1,2,3), Didier Neau (3), François Dabis (1,2,3), Philippe Morlat (1,2,3), Fabrice Bonnet (1,2,3), Geneviève Chêne (1,2,3) and the ANRS CO3 Aquitaine Study Group (1) INSERM, Bordeaux School of Public Health (ISPED), Centre INSERM U897 & CIC-EC7, F-33000 Bordeaux, France(2) Univ. Bordeaux, ISPED, Centre INSERM U897, F-33000 Bordeaux, France(3) CHU de Bordeaux, F-33000 Bordeaux, France(4) CHU de Bordeaux, F-33000 Pessac, France Type 2 diabetes is associated with lower cognitive performances in a cohort of HIV-infected patients. ANRS CO3 Aquitaine Cohort, Bordeaux, France, 2007-2009
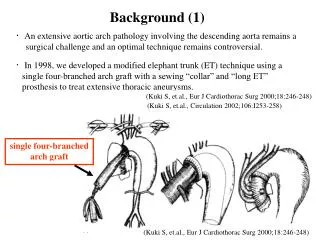
Background (1) • HIV-infected patients receiving combination antiretroviral therapy • Higher prevalence of vascular risk factors : hypercholesterolemia, diabetes, smoking • Higher risk of cardiovascular morbidity • Accelerated/accelerated aging notably of cognitive functions • Link between cardiovascular risk factors and cognition • Well established from studies on population-based studies on ageing • Rarely investigated in HIV-infected cohorts
Background (2) • Type 2 Diabetes : heterogeneous metabolic disorder • Reduced insulin sensitivity and relative insulin deficiency • Pre-diabetes (intermediate hyperglycemia) • High risk state for diabetes • Insulin resistance and b-cell dysfunction • Target organs • Kidney, eyes, arteries, heart • Brain : • Accelerated cognitive decline (main domains: executive functions, psychomotor speed and attention) • Risk of Alzheimer's disease : 50-100% higher in T2 diabetics
Objectives • In a large hospital-based cohort of HIV infected patients, the ANRS-CO3 Aquitaine cohort, to evaluate the association between • Diabetes and cognitive function at baseline and over time • Pre-diabetes and cognitive function at baseline and over time
Methods (1) • ANRS CO3 Aquitaine Cohort • Patients recruited through a hospital-based information system on HIV-1 infection in the Bordeaux University Hospital (Aquitaine region, South Western France) since 1987 • In- or out-patients of the participating hospitals • HIV-1 infection confirmed by Western blot testing • Informed consent signed • Sub-study on cognition • Baseline 2007-2009, Follow-up at 2 years • No acute opportunistic infection or cancer under treatment • 400 adult patients included • Follow-up at2-years : 288 participants
Methods (2) • Assessment of several cognitive domains • "Trail making test" : Attention and executive functions • "Digit Symbol Substitution test" : Psychomotor speed • "Purdue Pegboard Test" : Manual dexterity and coordination • "Rey complex figure test" : Visuospatial abilities • "Digit span" : Working memory • "Grober & Buschke" : Episodic memory • "Isaac Set Test" : Semantic Fluency • Categories for glycaemia status • Diabetes : at least two glycaemia >7 mmol/L or at least one glycaemia >11.1 mmol/L or use of anti-diabetic drug prior inclusion • Impaired glycaemia : at least two measures of glycaemia between 6.1 and 7 mmol/L prior inclusion • Normal : otherwise
Methods (3) • Polytomous logistic regression computed to investigate the association between glycaemia status and neurocognitive impairment categories (Revisedresearchcriteria for HIV-associated neurocognitive disorders; Frascati, 2007) • Covariance analysis computed to investigate the association between glycaemia status and • Raw cognitive test scores • Annualized percentage of change in cognition • Adjusting for age, gender, education, depression, HIV transmission category, CD4+ lymphocytes count, HIV-RNA, exposure to ART (including Stavudine, Didanosine, Indinavir), AIDS stage, and hypertension, hypercholesterolemia, BMI, smoking status • Inverse probability weighting to correct for attrition
Baseline characteristics - 26 treated - 12 elevated glyc. levels
Glycaemia status according to neurocognitive impairment at baseline • Prevalence of neurocognitive impairment • Asymptomatic neurocognitive disorders (ANI): 21.0% (n=84) • Mild neurocognitive disorder (MND): 32.0% (n=126) • HIV-associated dementia (HAD): 6.7% (n=27) P=0.44, in multivariable analyses
Trail Making Test (part B) Performance at Trail Making Test B is measured through a time to perform a task. The higher the time, the worse the performance
Cognitive performances distribution No significantchange
Multivariablemodelsadjusted for age, gender, education, depression, HIV transmission category, CD4+ lymphocytes count, HIV-RNA, exposure to ART (current and past, including Stavudine, Didanosine, Indinavir), AIDS stage, and hypertension, hypercholesterolemia, BMI, smoking status Cross-sectional analyses
Multivariablemodelsadjusted for baselineage, gender, education, depression, HIV transmission category, CD4+ lymphocytes count, HIV-RNA, exposure to ART (current and past, incl. Stavudine, Didanosine, Indinavir), AIDS stage, and hypertension, hypercholesterolemia, BMI, smoking status Longitudinal analyses: annualizedpercentage of change
Adjustedmeans of annualizedpercentage of change by glycaemiastatus
Adjustedmeans of annualizedpercentage of change by glycaemiastatus
Adjustedmeans of annualizedpercentage of change by glycaemiastatus • No change in findingsafterusing inverse probabilityweighting to takeintoaccount attrition
Conclusion & perspectives (1) • In summary • Largeststudywithfollow-up available • Diabetic patients performworse on average on cognitive tests especiallythoseassessingexecutivefunctions, attention and psychomotor speed • No association with other cardiovascular risk factors (results not shown) • Not evidenced when all categories of NCI are used • Published findings In HIV patients : • Diabetes and dementia (Valcour 2005) • Diabetes and NCI in older patients (McCutchan2012)
Conclusion & perspectives (2) • Potential mechanism • Brain Micro- or macro-vascular damages • Neuro-Inflammation • Implications for dailyclinicalpractice • Detectand control diabetesat the earliest possible stage, • Healthylifestyle, limit prescription of ARV treatmentassociatedwithdiabetes • Future analyses • Impact of glycaemia control (glycaetedhemoglobin) and change in glycaemiastatus • Longer neurocognitive follow-up and brainimaging
ANRS CO3 Aquitaine Cohort Composition of the Grouped’Epidémiologie Clinique du Sida en Aquitaine (GECSA): Coordination: F. Dabis Scientificcommittee: F. Bonnet, S. Bouchet, F. Dabis, M. Dupon, G. Chêne, H. Fleury, V. Gaborieau, D. Lacoste, D. Malvy, P. Mercié, I. Pellegrin, P. Morlat, D. Neau, JL. Pellegrin, S. Tchamgoué, R. Thiébaut. Epidemiology and Methodology: M. Bruyand, G. Chêne, F. Dabis, S. Lawson-Ayayi, R. Thiébaut, L. Wittkop. Infectious Diseases and Internal Medicine: CHU de Bordeaux: P. Morlat (F. Bonnet, N. Bernard, M. Hessamfar, D. Lacoste, MA. Vandenhende) ; M. Dupon (FA. Dauchy, H. Dutronc) ; M. Longy-Boursier (P. Mercié, P. Duffau, J. Roger Schmeltz) ; D. Malvy (T. Pistone, MC Receveur) ; D. Neau (C. Cazanave, A. Ochoa, T. Pistone, MO. Vareil) ; JL. Pellegrin (JF. Viallard, C. Greib, E. Lazaro) CHG d’Arcachon : A. Dupont. CHG de Dax : Y. Gerard, K. André, L. Caunègre CHG de Bayonne : F. Bonnal, S. Farbos, MC. Gemain. CHG de Libourne : J. Ceccaldi, S. Tchamgoué CHG de Mont-de-Marsan : S. De Witte, C. CourtaultCHG de Pau : E. Monlun, V. Gaborieau CHG de Périgueux : P. Lataste, JP. MeraudCHG de Villeneuve-sur-Lot : I. Chossat. Immunology: JF. Moreau, I. Pellegrin. Virology: H. Fleury, ME. Lafon, B. Masquelier, P. Trimoulet. Pharmacology: D. Breilh, S. Bouchet, M. Molimard, K. Titier. Drug monitoring: F. Haramburu, G. Miremont-Salamé. Data collection and processing: MJ. Blaizeau, M. Decoin, J. Delaune, S. Delveaux, C. D’Ivernois, C. Hanappier, O. Leleux, E. Lenaud, B. Uwamaliya-Nziyumvira, X. Sicard. Computing and Statistical analysis: V. Conte, A. Frosh, S. Geffard, J. Leray, I. Louis, G. Palmer, D. Touchard. Members of the GECSA-COGLOC Study Group: M. Allard, H. Amieva, M. Auriacombe, S. Auriacombe, E. Bestaven, F. Bonnet, M. Bruyand, M. Campoy, G. Catheline, G. Chêne, G. Coldefy, F. Dabis, J.-F. Dartigues, F.-A. Dauchy, S. Delveaux, P. Dehail, C. Dufouil, C. Greib, C. Lewden, J. Macua, F. Marquant, F. Matharan, P. Mercié, C. Milien, P. Morlat, N. Raoux, L. Richert.