Download
1 / 1
10 likes | 110 Vues
Biopsy showing clearing of cytoplasm. Post Operative PET scan Nodal metastases marked. Repeat PET scan at 6mths. No. 203. Doctor, why is it hard to pee? Clear cell adenocarcinoma (CCA) in a female urethral diverticulum. Dr Guy Sheahan MBBS, Dr Antonio Vega Vega MBBS PhD FRACS( Urol ).

E N D
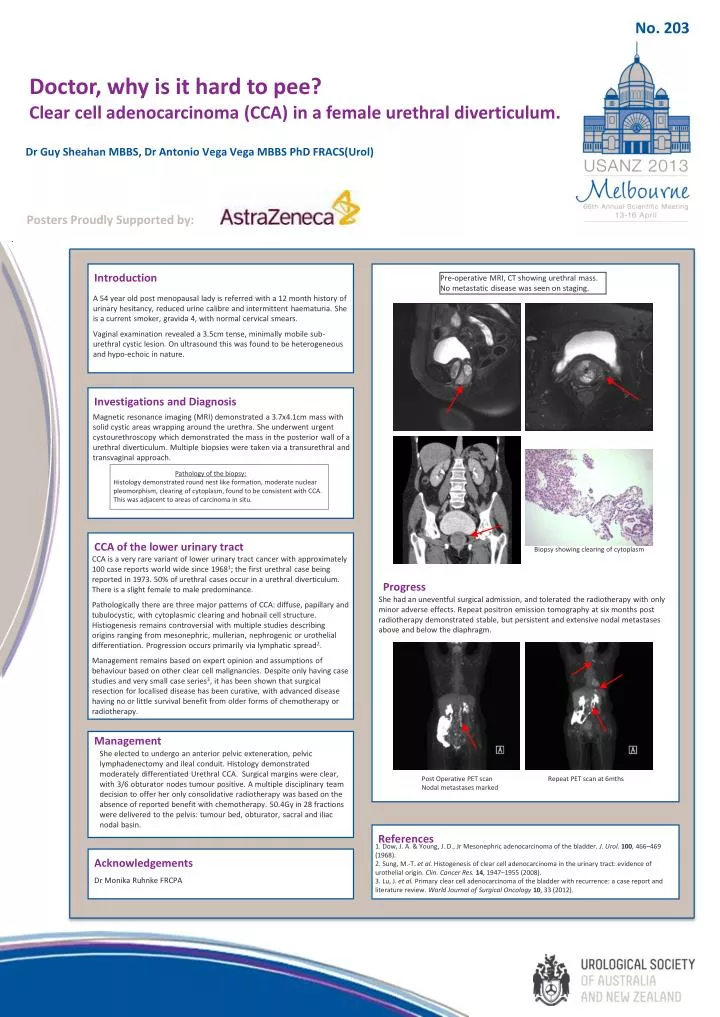
Biopsy showing clearing of cytoplasm Post Operative PET scan Nodal metastases marked Repeat PET scan at 6mths No. 203 Doctor, why is it hard to pee? Clear cell adenocarcinoma (CCA) in a female urethral diverticulum. Dr Guy Sheahan MBBS, Dr Antonio Vega Vega MBBS PhD FRACS(Urol) Posters Proudly Supported by: Introduction Pre-operative MRI, CT showing urethral mass. No metastatic disease was seen on staging. A 54 year old post menopausal lady is referred with a 12 month history of urinary hesitancy, reduced urine calibre and intermittent haematuria. She is a current smoker, gravida 4, with normal cervical smears. Vaginal examination revealed a 3.5cm tense, minimally mobile sub-urethral cystic lesion. On ultrasound this was found to be heterogeneous and hypo-echoic in nature. Investigations and Diagnosis Magnetic resonance imaging (MRI) demonstrated a 3.7x4.1cm mass with solid cystic areas wrapping around the urethra. She underwent urgent cystourethroscopy which demonstrated the mass in the posterior wall of a urethral diverticulum. Multiple biopsies were taken via a transurethral and transvaginal approach. Pathology of the biopsy:Histology demonstrated round nest like formation, moderate nuclear pleomorphism, clearing of cytoplasm, found to be consistent with CCA. This was adjacent to areas of carcinoma in situ. CCA of the lower urinary tract CCA is a very rare variant of lower urinary tract cancer with approximately 100 case reports world wide since 19681; the first urethral case being reported in 1973. 50% of urethral cases occur in a urethral diverticulum. There is a slight female to male predominance. Pathologically there are three major patterns of CCA: diffuse, papillary and tubulocystic, with cytoplasmic clearing and hobnail cell structure. Histiogenesis remains controversial with multiple studies describing origins ranging from mesonephric, mullerian, nephrogenic or urothelial differentiation. Progression occurs primarily via lymphatic spread2. Management remains based on expert opinion and assumptions of behaviour based on other clear cell malignancies. Despite only having case studies and very small case series3, it has been shown that surgical resection for localised disease has been curative, with advanced disease having no or little survival benefit from older forms of chemotherapy or radiotherapy. Progress She had an uneventful surgical admission, and tolerated the radiotherapy with only minor adverse effects. Repeat positron emission tomography at six months post radiotherapy demonstrated stable, but persistent and extensive nodal metastases above and below the diaphragm. Management She elected to undergo an anterior pelvic exteneration, pelvic lymphadenectomy and ileal conduit. Histology demonstrated moderately differentiated Urethral CCA. Surgical margins were clear, with 3/6 obturator nodes tumour positive. A multiple disciplinary team decision to offer her only consolidative radiotherapy was based on the absence of reported benefit with chemotherapy. 50.4Gy in 28 fractions were delivered to the pelvis: tumour bed, obturator, sacral and iliac nodal basin. References 1. Dow, J. A. & Young, J. D., JrMesonephric adenocarcinoma of the bladder. J. Urol.100, 466–469 (1968). 2. Sung, M.-T. et al.Histogenesis of clear cell adenocarcinoma in the urinary tract: evidence of urothelial origin. Clin. Cancer Res.14, 1947–1955 (2008). 3. Lu, J. et al. Primary clear cell adenocarcinoma of the bladder with recurrence: a case report and literature review. World Journal of Surgical Oncology10, 33 (2012). Acknowledgements Dr Monika Ruhnke FRCPA