Download
1 / 47
470 likes | 602 Vues
TREATMENTS OTHER THAN CPAP; PHARMACOLOGICAL TREATMENT. Prof. Turan Acıcan MD Medical School of Ankara University, Dept. of Pulmonary Diseases. Medical Therapy for Obstructive Sleep Apnea Hypopnea Syndrome. BEHAVIORAL INTERVENTIONS Weight Loss Smoking Cessation Music

E N D
TREATMENTS OTHER THAN CPAP; PHARMACOLOGICAL TREATMENT Prof. Turan Acıcan MD Medical School of Ankara University, Dept. of Pulmonary Diseases
Medical Therapy for Obstructive Sleep Apnea Hypopnea Syndrome BEHAVIORAL INTERVENTIONS • Weight Loss • Smoking Cessation • Music • Sleep Hygiene and Sleep Deprivation • Body Position • Alcohol • Sedatives • Narcotics and Anesthetics • Barbiturates
Smoking Cessation • Cigarette users have more difficulty initiating and maintaining sleep and experience increased daytime sleepiness as well. • Smokers have fourfold to fivefold greater risk than that of never-smokers for having sleep-disordered breathing. Heavy smokers are at greatest risk. • Cigarette smoking may contribute to upper airway dysfunction during sleep by eliciting mucosal edema and increased upper airway resistance
Nicotine administered as gum reduces apnea frequency over the first several hours of sleep. The short duration of action precludes effective therapeutic application of nicotine gum for OSAHS. • There was no clinically significant reduction in disordered breathing event frequency after application of transdermal nicotine patches. • Adverse effects were observed in conjunction with the transdermal patch, including reduced total sleep time, sleep efficiency, and rapid eye movement (REM) sleep. • Other side effects, including gastrointestinal complaints, lightheadedness, and tremor, were also reported.
Sleep Hygiene and Sleep Deprivation • Sleep deprivation is associated with blunted hypoxic and hypercapnic ventilatory chemoresponsiveness during wakefulness, and may prolong apneas and hypopneas with consequently greater oxyhemoglobin desaturation by depressing the arousal response
Body Position • Manipulation of body position to promote sleeping in the lateral recumbent posture or with a 30- to 60-degree head elevation may lead to clinically significant improvement of OSAHS in a proportion of patients
Alcohol • Alcohol evokes obstructive apnea in individuals who otherwise only snore and increases the apnea frequency in patients with preexisting OSAHS . • Alcohol consumption increases the duration of these events. • Alcohol may also have a particularly adverse impact on daytime alertness in patients with OSAHS. • The hypnotic effect of this agent is enhanced in the presence of underlying sleepiness
The key message is that individuals with OSAHS, treated or untreated, would be best served by abstinence from alcohol. • Although this is prudent advice, not all patients will follow this directive. If a patient is unwilling to abstain completely, he or she should be told to limit the alcohol intake to small quantity, and not to consume alcohol for a time before bedtime that is sufficient to permit the blood alcohol level to fall to nil.
Sedatives • flurazepam has been the subject of several investigations. This agent may worsen OSAHS in some individuals who otherwise have minimal sleep-disordered breathing. • temazepam did not significantly increase the RDI or alter the degree of oxyhemoglobin desaturation compared with placebo. • In usual hypnotic doses, benzodiazepines may not present a substantial risk for evoking OSAHS in some otherwise normal individuals
Zolpidem • Assess the effect of the hypnotic zolpidem on the efficacy of nCPAP for treatment of Obstructive Sleep Apnea • 16 patients with severe obstructive sleep apnea (apnea+ hypopnea index > 30/hr), on CPAP therapy for at least 6 months • Acute administration of zolpidem 10 mg does not impair the efficacy of an effective level of CPAP in patients with severe obstructive sleep apnea Berry RB, Patel PB Effect of zolpidem on the efficacy of continuous positive airway pressure as treatment for obstructive sleep apnea.Sleep. 2006 Aug 1;29(8):1052-6
Narcotics and Anesthetics • There are reports of clinically significant upper airway obstruction developing after administration of intravenous narcotics(hydromorphone hydrochloride) • There are instances when humane medical practice requires analgesia, such as in the postoperative setting or during some procedures (e.g., bronchoscopy or colonoscopy). • If nonnarcotic or nonventilatory depressant agents cannot provide adequate pain control, minimal doses of narcotics should be administered with careful monitoring.
Barbiturates • Like alcohol, this class of agents selectively reduces the neural output through the hypoglossal nerve, reduces the tone of the upper airway dilator muscles, and predisposes to upper airway occlusion during sleep • It is prudent to avoid barbiturates in patients who are predisposed to, or are known to have sleep-disordered breathing.
ENDOCRINE CONSIDERATIONS;HYPOTHYROIDISM • Hypothyroidism reflecting a risk factor for the OSAHS. • Patients with OSAHS may benefit from thyroid replacement therapy with a reduction of apnea frequency • Hypothyroid patients should be specifically interviewed and examined to detect factors that raise the probability that OSAHS is present. • Pelttari L, Rauhala E, Polo O, et al: Upper airway obstruction in hypothyroidism. J Intern Med 1995;236:177-181.
Grunstein et al. made the important observation that thyroid replacement therapy in patients with untreated OSAHS may precipitate cardiac complications attributable to ischemia in the setting of augmented metabolism and persistent nocturnal hypoxemia. • For this reason, as well as the benefit of more rapid relief of OSAHS, the authors suggested treatment with nasal CPAP(or successful oral appliance therapy) during thyroid replacement therapy.
The utility of screening unselected patients with OSAHS for hypothyroidism is controversial. • Winkelman and coworkers have reported a similar prevalence of chemical hypothyroidism in patients with OSAHS and individuals without OSAHS Winkelman JW, Goldman H, Piscatelli N, et al: Are thyroid function tests necessary in patients with suspected sleep apnea? Sleep 1996;19:790-793.
Estrogen and Progesterone • The effect of gender on OSAHS has been well defined, indicating a male-to-female ratio of 2:1 or 3:1. The postmenopausal state increases the risk of OSAHS. • The exact mechanisms are incompletely understood, but appear to be in part due to estrogen and progesterone levels. Jordan AS, McEvoy RD: Gender differences in sleep apnea: Epidemiology, clinical presentation and pathogenic mechanisms [see comment]. Sleep Med Rev 2003;7:377-389.
HRT • Recent reports have demonstrated that hormonal replacement therapy (HRT) has a favorable effect on the OSAHS. Shahar E, Redline S, Young T, et al: Hormone replacement therapy and sleep-disordered breathing [see comment]. Am J Respir Crit Care Med 2003;167:1186-1192. White DP: The hormone replacement dilemma for the pulmonologist [comment]. Am J Respir Crit Care Med 2003;167: 1165-1166.
HRT • The Heart and Estrogen/Progestin Replacement Study II (HERS II) and Women's Health Initiative (WHI) failed to demonstrate a favorable effect of HRT on cardiovascular risk. • In HERS II, there was a twofold risk of venous thromboembolism and a 50% increase in the rate of gallbladder disease that required surgery. • The estrogen/progestin arm of the WHI study was prematurely halted after 5.2 years of follow-up because of an increased risk of invasive breast cancer Paoletti R, Wenger NK: Review of the International Position Paper on Women's Health and Menopause: A comprehensive approach. Circulation 2003;107:1336-1339. Grady D, Herrington D, Bittner V, et al: Cardiovascular disease outcomes during 6.8 years of hormone therapy: Heart and Estrogen/progestin Replacement Study follow-up (HERS II). JAMA 2002;288;49-57.
HRT • Although a favorable effect of HRT on OSAHS has been demonstrated in postmenopausal women, the additional risks cited previously outweigh the potential benefit. • Further research may define subsets of patients and dosing regimens that are safe and effective. White DP: The hormone replacement dilemma for the pulmonologist [comment]. Am J Respir Crit Care Med 2003;167: 1165-1166.
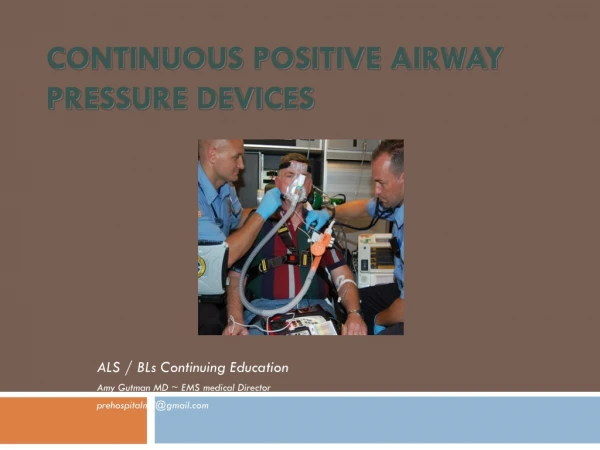
PHARMACOLOGIC INTERVENTIONS OXYGEN • In addition to sleep fragmentation, many of the consequences of OSAHS are associted with nocturnal hypoxemia. • Prevention of hypoxemia is therapeutic goal in patients with OSAHS. • Several older studies reported that administration of supplemental oxygen to patients with OSAHS may significantly increase apnea duration with associated hypercapnia and respiratory acidosis.
Martin et al. observed an initial prolongation of apnea duration in a group of eucapnic patients with OSAHS in conjunction with a significant reduction in apnea frequency. • This resulted in decreased apnea time and maintenance of satisfactory oxyhemoglobin saturation over the study period • The bradycardia that accompanied apnea was eliminated by supplemental oxygen administration.
Mean percent apnea time for eight patients (closed squares, solid line) and the average nadir of oxyhemoglobin saturation per apnea (open squares, dashed line) for each 7.5-minute interval during the three study conditions (Room Air I, Oxygen, Room Air II). Martin RJ, et al: Am Rev Respir Dis 1982;125:175-180.)
Gold and coworkers reported that supplemental oxygen was associated with a statistically, but not clinically significant reduction of apnea frequency, particularly during NREM sleep, as well as improved oxyhemoglobin saturation. • Apnea duration increased slightly by an average of 4 to 7 seconds across the study group. • There was no improvement in subjective or objective measures of daytime sleepiness during the period of nocturnal oxygen supplementation. • The evidence suggests that, supplemental oxygen during sleep is not sufficiently effective in reducing apnea frequency and increasing daytime alertness to stand alone as therapy for most patients Gold AR, Schwartz AR, Bleecker ER, Smith PL: The effect of chronic nocturnal oxygen administration upon sleep apnea. Am Rev Respir Dis 1986;134:925-9
Patients with coronary artery disease or cerebrovascular disease and slightly elevated frequency of abnormal breathing events during sleep, with unacceptable oxyhemoglobin desaturation during those events, might benefit from supplemental oxygen. • Monitoring important in patients with concomitant hypercapnia during wakefulness and is also necessary to determine the flow oxygen required for acceptable oxyhemoglobin saturation. Franklin KA, Nilsson JB, Sahlin C, Naslund U: Sleep apnoea and nocturnal angina. Lancet 1995;345:1085-1087
In addition to sole therapy in selected patients with OSAHS, oxygen may be a useful adjunct to CPAP. • Patients with OSAHS who are sufficiently hypoxemic during wakefulness to warrant oxygen therapy usually meet the criteria for this therapy during sleep, even if positive airway pressure treatment maintains upper airway patency. • It should be determined if persistent desaturation on CPAP is related to hypoventilation. • Bilevel positive pressure may permit sufficient reduction of expiratory pressure to avoid significant hypoventilation and desaturation and obviate the need for supplemental oxygen
O(2) supplementation to CPAP • Using a 3-arm placebo-controlled design, OSA patients (N = 38) were monitored 2 nights with polysomnography and then randomized to 2-weeks therapeutic CPAP, placebo CPAP, or O(2) supplementation. • Global Severity Index (GSI): significant reductions in GSI with O(2) supplementation and therapeutic CPAP, but not placebo CPAP. • Depression decreased with O(2) supplementation but not with therapeutic CPAP or placebo CPAP. • Both therapeutic CPAP and O(2) supplementation resulted in decreased psychological symptoms. Results suggest hypoxemia may play a stronger role than sleep disruption in OSA related psychological distress. Bardwell WA et al. Effects of 2-week nocturnal oxygen supplementation and continuous positive airway pressure treatment on psychological symptoms in patients with obstructive sleep apnea: a randomized placebo-controlled study. Behav Sleep Med. 2007;5(1):21-38.
Transtracheal Oxygen Delivery • Several studies have described the impact of transtracheal oxygen administration to patients with OSAHS. • If the transtracheal route of oxygen delivery is effective and superior to nasal cannulae in reducing OSAHS, it could be the result of stimulation of flow- or temperature-sensitive receptors in the upper airway. • The frequency and severity of complications resulting from transtracheal oxygen therapy in a predominantly obese patient population have not been well characterized • At present, transtracheal oxygen should be considered investigational in the treatment of patients with OSAHS.
Psychotrophic Agents (Anxiolytics and Hypnotics) Protriptyline • The tricyclic antidepressant protriptyline may reduce OSAHS by reducing the duration of REM sleep and by increasing the tone of the upper airway dilator muscles with increased hypoglossal and recurrent laryngeal nerve activity • Although protriptyline administration may result in a statistically significant reduction in sleep-disordered breathing events in study populations, breathing and oxygenation during sleep generally remain abnormal.
Patients with OSAHS receiving protriptyline report subjective improvement in daytime sleepiness despite a persistently elevated arousal frequency • Protriptyline has a number of side effects vary in severity and may limit use. They include dry mouth, urinary hesitancy, constipation, confusion, and ataxia • Because of its lack of clinically significant therapeutic impact and potentially troublesome side effects, protriptyline is not considered to be a standard intervention in the treatment of OSAHS.
Serotonin Uptake Inhibitors • Serotonin may mediate both upper airway dilator muscle and diaphragm activity. • It has been further postulated that the reduction in upper airway dilator muscle tone, particularly during REM sleep, is due to withdrawal of serotonin-related excitatory input to the hypoglossal motor neurons. • If these postulates are true, it could have substantial implications for the treatment of patients with OSAHS.
Buspirone • is a clinically available anxiolytic agent, the mechanism of action is believed to be mediated through serotonin receptors in the central nervous system. • Several animal studies have suggested that administration of buspirone augments ventilation during wakefulness and sleep and enhances ventilatory responsiveness to carbon dioxide. • In addition, the apneic threshold for carbon dioxide is reduced by an average of 3.7 mm Hg. • These data suggest that as a class of agents, serotonin agonists may have a therapeutic role in OSAHS
fluoxetine • Other serotonin agonists have been evaluated to limited degrees. After administration of 20 mg/day of, one study found a statistically significant reduction in the apnea plus hypopnea frequency, from 57 ± 9 to 34 ± 6 (mean ± SE), although there was wide intersubject variability and there was no significant impact on the arousal frequency. Hanzel DA, Proia NG, Hudgel DW: Response of obstructive sleep apnea to fluoxetine and protriptyline. Chest 1991;100: 416-421.
Several studies were published in the 1980s that reported the impact of l-tryptophan in the treatment of OSAHS. • It was subsequently observed that l-tryptophan has an unacceptable safety profile and should not be used because of its association with development of the eosinophilia-myalgia syndrome.
Mirtazapine • A mixed 5-HT2/5-HT3 antagonist that also promotes serotonin release in the brain would effectively reduce AHI during both NREM and REM sleep in patients with OSA. • Daily administration of 4.5 to 15 mg of mirtazapine for 1 week reduces AHI adult patients with OSA. These findings suggest the therapeutic potential of mixed-profile serotonergic drugs in OSA and provide support for future studies with related formulations. • Mirtazapine also is associated with sedation and weight gain–2 negative side effects in patients with OSA. • Because of the side effects, do not recommend use of mirtazapine as a treatment for OSA. Carley DW et al. Sleep. 2007 Jan 1;30(1):35-41.
Use of Medications to Promote Wakefulness • There are patients on adequate treatment to reverse upper airway dysfunction and maintain acceptable oxyhemoglobin saturation as well as sleep continuity, may still complain of disturbing diurnal sleepiness or lack of alertness. • Some patients remain unacceptably and perhaps dangerously sleepy or inattentive.
Recent animal data have demonstrated that long-term intermittent hypoxia (LTIH) can result in oxidative injury to the sleep-wake regions of the brain. • After the withdrawal of LTIH, objective sleepiness persisted, supporting the notion that sleepiness associated with sleep apnea may not be completely reversible Veasey SC, Davis CW, Fenik P, et al: Long-term intermittent hypoxia in mice: Protracted hypersomnolence with oxidative injury to sleep-wake brain regions. Sleep 2004;27:194-201.
Amphetamines • have been the class of agents used as stimulants. Unfortunately, this group of drugs has considerable potential for harmful cardiovascular consequences as well as adverse psychiatric and sleep effects
Modafinil • is an agent that is thought to be a central alpha1-adrenergic agonist with possible dopaminergic properties • Limited studies have suggested that modafinil increases daytime alertness and memory performance without significant side effects in patients without and with OSAHS Arnulf I, et al: Modafinil in obstructive sleep apnea-hypopnea syndrome: A pilot study in 6 patients. Respiration 1997;64: 159-161. .
Modafinil has recently been approved by the U.S. FDA for the treatment of residual sleepiness in OSAHS adequately treated with positive pressure by mask. • The most common side effects were headache (28%), anxiety (16%), and nervousness (14%).
In a 12-week open-label study involving 125 patients, improvements in subjective daytime sleepiness and sleep-related functional status were maintained. • There was a statistically significant decrease in CPAP use from 6.3 ± 1.3 hours per night at baseline to 5.9 ± 1.4 hours per night at the 12-week point, suggesting that modafinil may adversely affect adherence to CPAP. Schwartz JR, Hirshkowitz M, Erman MK, Schmidt-Nowara W: Modafinil as adjunct therapy for daytime sleepiness in obstructive sleep apnea: A 12-week, open-label study. Chest 2003;124:2192-2199
Armodafinil • 12-week, multicenter, double-blind, randomized, placebo-controlled study was conducted at 37 centers in the United States and Canada. 395 Male and female patients aged 18 to 65 years with residual ES associated with OSAHS were enrolled. Patients were randomly assigned to receive armodafinil 150 or 250 mg or placebo PO for 12 weeks.
Armodafinil • In this selected population of patients with OSA/HS and residual ES despite effective treatment with nCPAP, • armodafinil PO used as an adjunct to nCPAP treatment was associated with improved wakefulness and overall clinical condition. • Clinical benefit was shown at the first assessment and maintained for the 12-week duration of the study. • Armodafinil was also associated with significantly reduced interference of ES with daily activities and global fatigue. Armodafinil was well tolerated, with no adverse effect on nighttime sleep or nCPAP use. Roth T. Et al. Effects of armodafinil in the treatment of residual excessive sleepiness associated with obstructive sleep apnea/hypopnea syndrome: a 12-week, multicenter, double-blind, randomized, placebo-controlled study in nCPAP-adherent adults.Clin Ther. 2006 May;28(5):689-706.
Nasal dilators • Although the therapeutic benefit remains controversial, approximately 10% of patients with snoring and apnea have been reported to improve after administration of mucosal vasoconstrictors.
Conclusion • CPAP, oral appliances, and surgery are usually used as primary treatment in patients with OSAHS, • Other medical interventions play a role in management • Behavioral interventions involving avoidance of sleep deprivation, fitness, smoking cessation should be pursued, when appropriate, in all patients • Weight loss might ameliorate or completely reverse obstructive sleep apnea in obese patients. • alcohol and some drugs such as hypnotic sedatives and opiates may worsen episodes of apnea, such drugs should be avoided.
Conclusion • Neither drugs that may stimulate breathing, such as progestational agents and methylxanthines, nor medications used in an attempt to increase upper airway patency (e.g., antidepressants) have been demonstrated to be efficacious • Estrogen-progesterone combinations may be effective in selected menopausal patients with sleep apnea, but not as sole treatment. • The current evidence indicates that the benefit of chronic HRT for the purpose of improving OSAHS is outweighed by the potential risk of other medical complications. It is unknown whether alternate preparations or dosing regimens will favorably modify these significant medical risks.
Conclusion • Modafinil and armodafinil a wake-promoting medication, may play a role in treating residual sleepiness in patients compliant with CPAP therapy. • Oxygen has not been shown to be efficacious as a primary treatment of obstructive sleep apnea, but it may have a role in patients with obstructive sleep apnea who demonstrate severe hypoxemia during sleep but who do not tolerate any other therapy. • Oxygen should be used cautiously in this setting because it may prolong episodes of apnea.
Conclusion • The principal medical therapy for OSAHS remains positive pressure administered through a mask .Oral appliances can be useful in selected patients who cannot tolerate CPAP; • Other medical options may be important as adjuncts to these treatment options or as therapeutic interventions alone if the patient cannot accept or tolerate CPAP or oral appliance therapy as a primary treatment. Strollo PJ, Atwood CW, Sanders MH. Principles and practice of sleep med. www.sleepmedtext.com. 12 April 2007:1052-1065