Inhaler technique
Inhaler technique. Why is it important?. Essential to ensure patients are receiving inhaled medications May prevent basic treatment failure Correct device for patient may improve symptom management


Inhaler technique
E N D
Presentation Transcript
Why is it important? • Essential to ensure patients are receiving inhaled medications • May prevent basic treatment failure • Correct device for patient may improve symptom management • We wouldn’t let a patient put a tablet in their ear, what's the difference of letting them have bad inhaler technique?
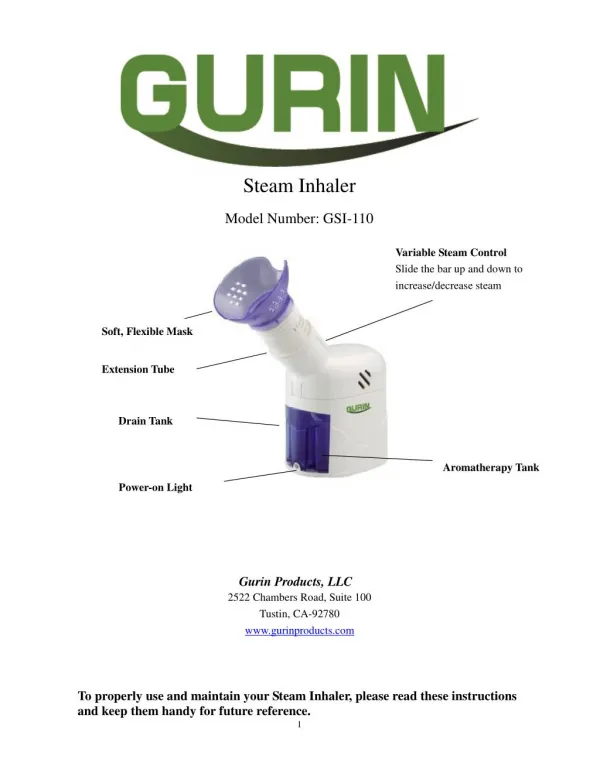
Liquid medication in aerosols or dry powder preparation for delivery via the mouth to enter the airways and act topically Depends on patient effort Depends on patient technique 90 degree angle How do they work?
Has been used since 1956 Regarded as “easy to use” 75% of patients have them (Pearce 2000) 50% are unable to use them (Hilton 1990) Those that can often forget with time or under stress Metered dose inhalers (MDIs)
Improves lung deposition Improves coordination of inhalation and delivery Often easier Gentle breathing Pharyngeal deposition greatly reduced Available with a mask for patients who can not form a good seal NO WHISTLE!! MDI and spacer
Primed and ready when cap is removed Spring mechanism is triggered by adequate inspiratory effort Not compatible with a spacer Easibreathe
Powder medication Requires patient inspiratory effort Easy to load Counter of doses window Accuhalers
Dry powder No propellant Requires patient effort Not compatible with spacer Requires breath hold Window with dose information Twist the base in both directions to load Turbohalers
Contains less propellant than an MDI. Breath activated Reduces issues between co coordinating dose initiation and breath Difficult to know when the inhaler is empty Dexterity problems Autohaler
Requires good inspiratory effort Dexterity needed to load device Must pierce tablet 24hr medication Make sure they don’t swallow the tablet! Handihalers
Dexterity to load device Spring loaded , good for those with poor inspiratory effort Fine powder particles Reduced cough More expensive 2 puffs OD Respimat
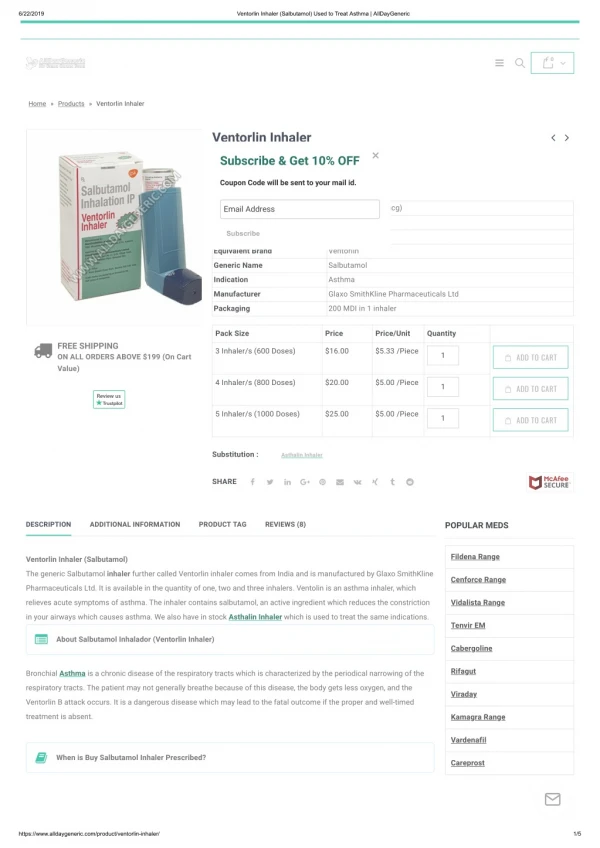
What do all these inhalers do? • Short acting beta 2 agonists • Colour coded blue “reliever/rescue” inhaler Acts on the beta 2 adrenergic receptor Dilates the bronchial passages Works within 5-20 mins, lasts approx 4 hours Side effects: tremor, tachycardia, headache Examples: Ventolin (salbutamol) Bricanyl (terbutaline)
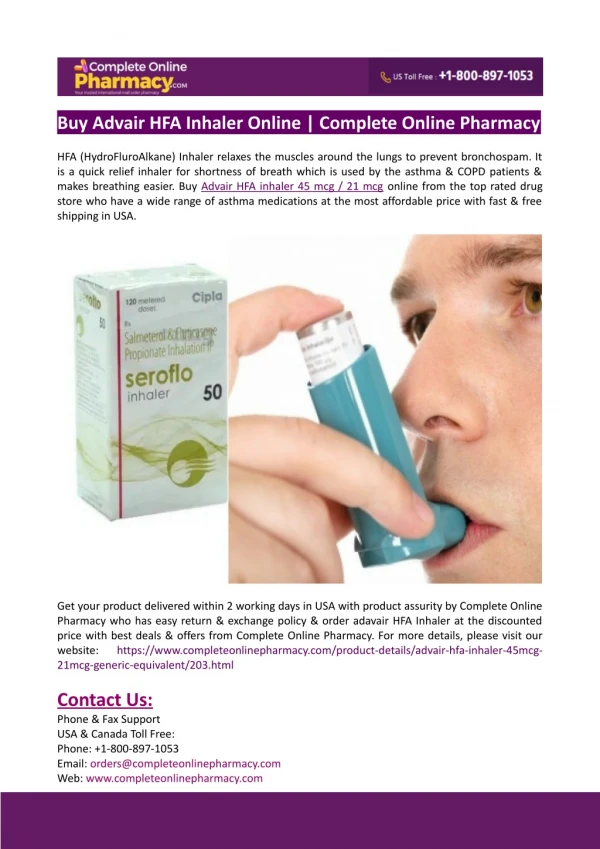
Long acting beta 2 agonists • Has same broncodilator effect • Has approx 12 hour effect • For continuous symptom control • Indicated for severe asthma and COPD • Colour coded green • Examples: Serevent (salmeterol)
Inhaled Corticosteroids • To topically treat the inflammation in the airways • Colour coded: usually brown • Examples: beclomethosone, pulmicort (budesonide) • Side effects: oral thrush, cough, hoarseness ALWAYS ADVISE PATIENT TO RINSE MOUTH AFTER USE
Combination Inhalers • Include; long acting beta 2 agonist and inhaled corticosteroid • Used as a combination maintenance inhaler to reduce inflammation and provide long-lasting bronchodilator effect • examples; Symbicort (budesonide/formoterol) RED • Seretide (fluticasone/salmeterol) PURPLE • AS PREVIOUS ALWAYS ADVISE PATIENT TO RINSE MOUTH POST USE
Quiz What inhaler would you recommend to a patient with left sided facial weakness? Why would you not give a patient with poor dexterity an MDI? How could you increase a patients medication delivery if they had an MDI What misconceptions do patients often have about turbohalers? How often should a COPD patient take their purple or red inhaler? What must a patient do with their handihaler before administration? What should you advise all patients to do with a combination/ steroid inhaler? Which inhalers can help if the patient has poor coordination?