Download

1 / 61
620 likes | 763 Vues
The role of sexual differences in function and physiological responses of women to exercise. Sexual dimorphism in exercise physiology Introduction Importance and application Exercise CVS Comparison Differences Mechanisms Outcomes.

E N D
The role of sexual differences in function and physiological responses of women to exercise
Sexual dimorphism in exercise physiology • Introduction • Importance and application • Exercise • CVS • Comparison • Differences • Mechanisms • Outcomes
Eur J Sport Sci. 2014 Jul 14 Clin J Sport Med. 2014 Jul 9. Am J Physiol Heart Circ Physiol. 2014 Jun 20 Exerc Sport Sci Rev. 2014 Jul;42(3) RespirPhysiolNeurobiol. 2014 May 1 Exerc Sport Sci Rev. 2014 Jul 24. Ultrasound Med Biol. 2014 Jul 9. RespirPhysiolNeurobiol. 2013 Dec 1 Pflugers Arch. 2013 May;465(5) Percept Mot Skills. 2012 Oct;115(2) J Pain. 2012 Dec;13 Chest. 2012 Nov;142(5) ExercImmunol Rev. 2011;17 Biol Sex Differ. 2011 Aug 25 Int J Psychol. 2009 Aug;44 Br J Sports Med. 2009 Jul;43(7) Exerc Sport Sci Rev. 2008 Jul;36(3) Med Sci Sports Exerc. 2008 Apr;40(4) Med Sci Sports Exerc. 2008 Apr;40(4) J Soc Psychol. 2007 Feb;147(1)
Men and women feature numerous physiological and anthropometric differences under resting conditions. The impact of these differences during exercise are important. Exercise as a model of various clinical stresses induces similar hormonal and immunological alterations and may provide insight into more effective clinical approaches and treatments. Exercise rehabilitation for patient populations, exercise prescription for disease prevention in healthy individuals and training strategies for competitive athletes. Age and gender–related decline in physical activity is antithetical to public health goals.
Exercise physiology Physical activity-stress, (True rest ?) Coordinate adjustments (acute, chronic or training) Healthful, Harmful , Irrelevant Amount of muscle mass at work Intensity of effort Duration Type of contraction (isometric, rhythmic)
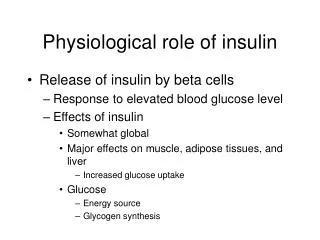
Skeletal muscle is an endocrine organ. J Pharmacol Sci. 2014 Jun 19;125(2):125-31. Epub 2014 May 23. Skeletal muscle: an endocrine organ. Clin Cases Miner Bone Metab. 2013 Jan;10(1):11-4. The regulation of interleukin-6 implicates skeletal muscle as an integrative stress sensor and endocrine organ. Exp Physiol. 2013 Feb;98(2):359-71.
Combination of neural and local factors 1- neural factors Central commands Muscle reflexes (mechanical/ metabolic) Baroreflex 2- Local factors Metabolic vasodilation
Quantification Maximal Oxygen Uptake (Vo2) Maximal Voluntary Contraction
1 km × 40 m × 10 m 300 gr × 75 years
Blood Flow Distribution During Rest and Dynamic Exercise in an Athlete Rest Heavy Exercise Area mL/min % mL/min % Splanchnic 1,400 24 300 1 Renal 1,100 19 900 4 Brain 750 13 750 3 Coronary 250 4 1,000 4 Skeletal muscle 1,200 21 22,000 86 Skin 500 9 600 2 Other 600 10 100 0.5 Total cardiac output 5,800 100 25,650 100
Numerous physiological and anthropometric differences exist between males and females: Absolute body size (men typically have larger hearts and brains than women) Body composition Muscle mass Blood volume Different organ structure and function independent of body size (female sex hormones )
Differences in peak VO2 in adolescent boys and girls disappear when peak VO2 is normalized to estimated leg muscle mass.
No sex differences in body weight response to exercise when energy expenditure is equivalent No sex differences in systolic blood pressure and heart rate responses to exercise after adjusting for exercise duration, body mass index (BMI), and resting SBP and HR. No sex differences in time to fatigue at 100% VO2 peak when normalized for fat free mass.
CVS responses Dynamic/Isometric (BP/Fatigue) Acute/Chronic (S, PS, muscle and respiratory pump)/ LV volume (Flow), LVH (Pressure) Respiratory responses Training has no effect
The degree of Intramuscular triacylglycerol (IMTG) hydrolysis during exercise is higher in women than in men. Sex differences in HSL expression, activity, and phosphorylation in skeletal muscle. HSL catalyze the hydrolysis of IMTG in skeletal muscle. Epinephrine increases skeletal muscle HSL activity both at rest and during contraction.
HSL specific activity during exercise is higher in men than in women, at least partly due to higher plasma epinephrine concentration in men resulting in higher HSL Ser659 phosphorylation. On the other hand, muscle HSL expression is higher in women than in men, which fully compensates the sex difference in HSL specific activity during exercise. Consequently, total HSL activity during exercise is similar in women and men and therefore cannot explain the higher IMTG net decrease during exercise in women compared with men. Rather, correlative analyses suggest that the higher IMTG hydrolysis during exercise in women than in men is at least partly explained by higher basal IMTG content in women. This could be due to improved enzyme-substrate interaction between IMTG and activated HSL in women.
Men’s and Women’s World Weightlifting Records as of 2006 for the Total Amount of Weight Lifted
Effects of Gender on Physiological Responses during Submaximal Exercise and Recovery V˙O2max is 5–15% lower in women than men even when expressed relative to body mass. This difference is reduced when V˙O2max is expressed relative to lean body mass. Other factors contributing to the lower V˙ O2max values observed among women include: decreased maximal cardiac output, stroke volume, and hemoglobin concentration and thus oxygen carrying capacity—of the blood delivered to the working muscle. When relative exercise intensity is held constant, men and women respond similarly, not only while exercising but also during recovery from that stressor for variables such as : HR, MAP, and temperature The gender-related differences are exist for these variables: greater systolic blood pressure, plasma volume shifts, RER values, and plasma lactate concentrations during exercise (in males). However, with the exception of plasma lactate, these differences were no longer evident during post exercise recovery.
* Significant difference between men and women at that time point.
* Significant difference between men and women at that time point. # Significant difference from pre exercise and 15-min post exercise in women, but not men.
The greater systolic pressures displayed by men are probably due to the enhanced stroke volumes and cardiac outputs noted among men during exercise which in turn are probably accounted for by differences in heart size between males and females. Interestingly, these gender-related disparities in systolic pressure during exercise were not reflected in MAP responses. This is best explained by exercise-induced responses in diastolic pressure. whereby women’s values exceeded those of men.
Men displayed higher RER values during exercise, suggesting a heavier reliance on carbohydrate utilization. This preference for carbohydrate catabolism would increase the activity of the glycolytic and glycogenolytic pathways, ultimately leading to greater lactate production by working muscles. This gender-related difference in lactate production may also be accounted for by evidence that, compared with females, the skeletal muscle tissue of men possesses enhanced glycolytic/glycogenolytic enzyme capacities.
Example calculation of sex differences in metabolic heat production during exercise at a fixed percentage of maximum oxygen consumption If a male and female perform exercise at 50% of their same relative ˙VO2max of 50 ml kg−1 min−1, exercise oxygen consumption would equal 25ml kg−1 min−1 in both cases. Assuming that the male weighs 70 kg and the female 60 kg, absolute oxygen consumption will equal 1750 ml min−1 for the male and 1500 ml min−1 for the female. Assuming a respiratory exchange ratio of 0.85 and the same external workload, the 250 ml min−1 difference between sexes will result in a rate of metabolic heat production that is ∼80–85W greater in the male. Such a difference in rate of metabolic heat production has been shown to result in proportional differences in whole-body heat loss
Sex differences in temperature regulation Females have a lower sudomotor activity, as well as a lower thermosensitivity compared to males during exercise performed at a fixed rate of metabolic heat production. The majority of studies generally focused on those related to the female menstrual cycle and differences in physical characteristics and rate of metabolic heat production. There is sex differences in sudomotor activity during exercise, independently of differences in physical characteristics and rate of metabolic heat production.
Left panel: an increase in mean body temperature occurs before the effector response is activated at a given onset threshold. The effector output subsequently increases proportionally to the increase in mean body temperature, the linear portion of which represents the thermosensitivity of the response. Once the effector response reaches maximal values, a flattening of the line is observed, whereby no further increase in effector output occurs despite increasing mean body temperature. Right panel: examples of how the parameters of the thermoeffector output-to-mean body temperature relationship can change: (1) the thermosensitivity of the response is increased, such that a greater change in effector output occurs for a given change in mean body temperature; (2) the onset threshold of the response is shifted to the right, such that a greater change in mean body temperature is required to initiate the activation of effector output; (3) the plateau phase of the effector output is reduced, such that lower maximal values are attained for a given change in mean body temperature.
Sexdifferences in exercise-induced cardiac hypertrophy. • Sex-related differences in muscle deoxygenation during exercise. • Sex differences in hemodynamic and arterial stiffness. • Sex differences in pulmonary function during exercise. • Sex differences in time to fatigue at 100% VO2 peak • Sex differences in exercise-induced muscle pain and muscle damage • sex-based differences in the effect of exercise on body weight • sex differences in in immune response to exercise. • sex differences in psychological effects of exercise. • Sex differences in the association between physical exercise and IQ.
Physical exercise have beneficial effects on cognitive performance Greater physical activity was associated with higher intelligence scores for women, whereas exercise level was essentially unrelated to intelligence among men. These associations remained consistent even after controlling for demographic and socioeconomic factors. The association between exercise and IQ appears to be moderated by sex in healthy adults, possibly through its effects on glucoregulation, insulin sensitivity, or other factors that differ between men and women.
Sex-related differences in muscle deoxygenation during exercise. women display a poorer ability to deliver O2 to the exercising tissue compared to men and oxidative demands must be supplemented by a greater fractional O2 extraction.
Differences in exercise-induced cardiac hypertrophy. Physiological cardiac hypertrophy (PCH), induced by intensive exercise or pregnancy. cardiac myocytes enlargement, with no apparent sign of fibrosis or apoptosis, and does usually not result in cardiac failure. Pathological myocardial hypertrophy (aortic stenosis ,chronic arterial hypertension).
Sex-specific differences in adipose tissue lipolysis and systemic fat metabolism induced by intensive training. Sex hormones, such as estrogens and testosterone, in addition to their role in the regulation of adipose tissue metabolism, were also reported to modulate development of myocardial hypertrophy
Changes in Blood Concentrations of Testosterone and Estrogen From Birth to Adulthood Whereas quantitative differences in hypertrophy and muscle gain exist that relative changes are similar. Thus young women have the capacity to hypertrophy their muscle fibers in response to resistance training , despite 10-fold lower testosterone concentration than men.
Sex differences in exercise-induced muscle pain and muscle damage. Sex differences in self-reported symptoms after aerobic exercise Women reported moderately lower and less frequent muscle pain than men. Both genders report increases in somatic symptoms (numbness, tingling ,…), but only women report decreases in emotional symptoms (irritability, sadness, nervousness,…).
Mechanics of breathing during exercise in men and women • Women have smaller airways and lung volumes, smaller diffusion surface and lower resting maximal expiratory flow rates relative to men. • Female athletes develop expiratory flow limitation more frequently than male athletes, and they have greater increases in end-expiratory and end-inspiratorylung volume at maximal exercise. • Women use a greater fraction of their ventilatory reserve and have a higher metabolic cost of breathing.
Women may be more prone to pulmonary limitations during heavy exercise (and perhaps submaximal intensities) than men due to the influence of the reproductive hormones (estrogen and progesterone) combined with a reduced pulmonary capacity. In particular, a greater ventilatory work associated with increased expiratory flow limitation during exercise and gas exchange impairments seem to be of primary concern.
Differences in Maximal Ventilatory Volumes With Age in Untrained (UT) and Trained (TR) Females and Males
Sex-related differences in the normal cardiac response to exercise About 30% of women demonstrated either a decrease in or a failure to increase ejection fraction during exercise. Normal middle-aged men and women achieve increases in stroke volume during exercise by different mechanisms. In men, a 23% increase in stroke counts resulted from an increase in ejection fraction with little or no change in end-diastolic counts, while in women a similar increase in stroke counts (33%) was achieved through an increase in end-diastolic counts without an increase in ejection fraction from rest to maximal exercise. These differences are related to sex rather than to variations in physical condition or motivation to exercise.
Women have a relatively reduced ability to increase left ventricular contractility in response to exercise stress compared with men of a similar age. Decreases in ejection fraction were accompanied by increases in end-diastolic counts, which is consistent with a compensatory increase in cardiac size that would be required to maintain stroke volume despite reduced systolic function.
The effects of sex on sympathetic neural control during static exercise in humans Estrogen and/or progesterone provide cardioprotection. Static exercise invokes increases in HR, BP, and muscle sympathetic nerve activity (MSNA) through two neural pathways: central command and the exercise pressor reflex. The exercise pressor reflex is a feedback system arising from mechano- (group III) and metabosensitive (group IV) afferent nerve endings within the skeletal muscle. This feedback loop increases BP through increases in MSNA, which is one determinant of vasoconstriction in nonexercising muscles. Baseline MSNA was comparable between the sexes. The low and high hormone phases of the menstrual cycle did not influence baseline MSNA. Women demonstrating a reduced metaboreceptor response, which is independent of exposure to low or high sex hormone concentrations. Women had lower concentrations of H+ and H2PO4- in the muscle ; H+ and H2PO4- have been positively associated with increases in MSNA. Women demonstrated a blunted metaboreflex, unaffected by sex hormones, which may be due to differences in muscle mass or fiber type and, therefore, metabolic stimulation of group IV afferents.
A: changes in muscle protein synthesis (MPS) and muscle protein breakdown (MPB) in response to feeding (i.e., amino acids). B: changes in MPS and MPB in response to resistance exercise and feeding.
SEX-BASED DIFFERENCES IN PROTEIN METABOLISM Exercise training and protein metabolism: influences of contraction, protein intake, and sex-based differences Muscle contraction during exercise, whether has profound affects on muscle protein turnover. It is well established that feeding during the postexercise period is required to bring about a positive net protein balance (muscle protein synthesis -muscle protein breakdown). Minor differences in muscle protein turnover appear to exist in young men and women; however, with aging there may be more substantial sex-based differences in response to both feeding and exercise. muscle protein synthesis (MPS) and muscle protein breakdown (MBP) contribute algebraically to defining the overall net protein balance (NPB MPS minus MPB). Feeding and exercise must be utilized concurrently to manifest a positive NPB, which will ultimately summate into skeletal muscle hypertrophy.