Download
1 / 82
820 likes | 858 Vues
Learn about lymphoma, its classifications, and diagnostic criteria as per the World Health Organization. Understand the clinical behaviors and frequency of lymphoid neoplasms.

E N D
LYMPHOMA- Non-Hodgkin lymphoma- Hodgkin lymphoma (Hodgkin disease) Agnieszka Tomaszewska Department of Hematology, Oncology and Internal Medicine, Medical University of Warsaw, 12 JAN 2006
Lymphoma - definition • Lymphoma (or malignant lymphoma) – a neoplasm of cells derived from lymphocytes or lymphocyte precursors • Lymphoma vs lymphoid leukemia: • Lymphoma – a neoplasm manifesting primarily as a tumor of lymph nodes or related organs (e.g. spleen, liver) • Leukemia – proliferation of abnormal cells (lymphocytes or lymphocytes precursors) in the bone marrow and blood
Normal lymph node architecture • Afferent lymphatic vessel • Sinus • Nodule (follicle): germinal center, mantle zone, marginal zone • Capsule • Medulla • Valve to prevent backflow • Efferent lymphatic vessel
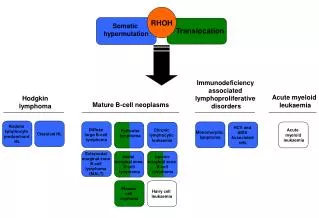
Principles of the classification of lymphoma • There are two main categories: • Non-Hodgkin lymphoma • B-cell lymphomas • T-cell lymphomas • Hodgkin disease (lymphoma)
The World Health Organization Classification of Lymphoid Neoplasms (2001) • B-cell neoplasms • Precursor B-cell neoplasms • Precursor B lymphoblastic leukemia/lymphoma (precursor B-cell acute lymphoblastic leukemia) • Mature (peripheral) B-cellneoplasms with leukemic presentation
The World Health Organization Classification of Lymphoid Neoplasms (2001) (cont.) • Mature (peripheral) B-cell neoplasms with leukemic presentation • Chronic lymphocytic leukemia (CLL)/B-cell small lymphocytic lymphoma (SLL) • B-cell prolymphocytic leukemia • Lymphoplasmacytic lymphoma (Waldenström’s Primary Macroglobulinemia) • Splenic marginal zone B-cell lymphoma (+/- villus lymphocytes) (SMZL)
The World Health Organization Classification of Lymphoid Neoplasms (2001) (cont.) • Mature (peripheral) B-cell neoplasms with leukemic presentation (cont.) • Hairy cell leukemia (HCL) • Plasma cell neoplasms • Extranodal marginal zone B-cell lymphoma of MALT type (MALT lymphoma)
The World Health Organization Classification of Lymphoid Neoplasms (2001) (cont.) • Mature (peripheral) B-cell neoplasms node-based • Nodal marginal zone B-cell lymphoma (MZL) • Follicular lymphoma (FL) • Mantle cell lymphoma (MCL) • Diffuse large B-cell lymphoma (DLBCL) • Burkitt’s lymphoma/leukemia • Lymphomatoid granulomatosis
The World Health Organization Classification of Lymphoid Neoplasms (2001) (cont.) • T-cell and NK-cell neoplasms • Precursor T-cell neoplasms • Precursor T lymphoblastic leukemia/lymphoma (precursor T-cell acute lymphoblastic leukemia) • Mature (peripheral) T-cell neoplasms with leukemic presentation
The World Health Organization Classification of Lymphoid Neoplasms (2001) (cont.) • Mature (peripheral) T-cell neoplasms with leukemic presentation • T-cell prolymphocytic leukemia • T-cell large granular lymphocytic leukemia • Aggressive NK-cell leukemia • Adult T-cell lymphoma/leukemia (HTLV1+)
The World Health Organization Classification of Lymphoid Neoplasms (2001) (cont.) • Mature (peripheral) T-cell neoplasms, various types of presentation • Extranodal NK/T-cel lymphoma, nasal type • Enteropathy-type T-cell lymphoma • Hepatosplenic T-cell lymphoma • Subcutaneous panniculitis-like T-cell lymphoma • Blastic NK-cell lymphoma
The World Health Organization Classification of Lymphoid Neoplasms (2001) (cont.) • Mature (peripheral) T-cell neoplasms, various types of presentation (cont.) • Mycosis fungoides/Sézary syndrome • Primary cutaneous CD30+ T-cell lymphoproliferative disorders • Peripheral T-cell lymphoma, unspecified • Angioimmunoblastic T-cell lymphoma • Primary systemic anaplastic large cell lymphoma
The World Health Organization Classification of Lymphoid Neoplasms (2001) (cont.) • Hodgkin’s lymphoma (Hodgkin’s disease) • Nodular lymphocyte predominant Hodgkin’s lymphoma • Classical Hodgkin’s lymphoma • Nodular sclerosis (most common) • Mixed cellularity • Lymphocyte depleted (extremely rare)
Grouping lymphomas by clinical behaviour • Indolent (slow growing) but usually incurable • CLL/SLL • FL except the large-cell type • Some MZL, gastric MALT lymphoma is often curable in the early stages
Grouping lymphomas by clinical behaviour • Fairly aggressive if untreated, but may becured with appropriate therapy • HD • FL large-cell type • DLBCL
Grouping lymphomas by clinical behaviour • Fairly aggressive and incurable • MCL • Extremely aggressive if untreated, but potentiallycurable with appropriate therapy • Burkitt lymphoma • Lymphoblastic lymphoma
Diagnosis of lymphoma • History • Age of the patient (pediatric/adult) • History of nodes (rapid, slow growth) • Pain • Local or systemic symptoms (unexplained fever, weight loss, night sweats) • Fatigue • Pruritus • Dermatosis, rash • Overall performance status
Diagnosis of lymphoma • Physical examination • Areas of palpable lymphadenopathy (size, location, tenderness) • Size of liver and spleen • Bony tenderness • Neurologic abnormalities
Diagnosis of lymphoma • Laboratory studies • CBC (complete blood count), differential and platelet count, • Erythrocyte sedimentation rate (esp. for HD) • Serum alkaline phosphatase, lactic dehydrogenase, albumin, uric acid • Renal function (creatinine, blood urea nitogen–BUN) tests • Liver function tests
Diagnosis of lymphoma • Radiologic studies • Chest radiograph • Computed tomography scan of the chest, abdomen and pelvis • Bone scan or radiograph if symptoms of bone involvement are present • Gallium or positron emission tomography (PET) scan, especially when other radiologic studies are equivocal
Diagnosis of lymphoma • Biopsies • Diagnostic biopsy of affected lymph node (reviewed by experienced hematopathologist !!!) • Bone marrow biopsy, especially when treatment may be modified • Biopsy of suspicious disseminated extranodal sites (e.g. pulmonary or liver lesions) if clinically indicated
Differential diagnosis of lymphadenopathy • Infections (such as common cold, local acute or chronic infections, infectious mononucleosis, tuberculosis, syphilis, toxoplasmosis, cytomegalovirus, HIV, cat-scratch fever) • Drugs (e.g. phenytoin) • Connective tissue disorders (e.g. systemic lupus erytematosus, dermatomyositis, scleroderma) • Metastatic cancer • Primary lymphoid malignancies (e.g. non-HL, HD)
Non-Hodgkin lymphomas – selected examples (clinical features, prognostic factors, staging systems, treatment) • CLL • FL • DLBCL • Mycosis fungoides/Sezary Syndrome
Chronic lymphocytic leukemia (B-cell CLL) • Most common leukemia in the Western Hemisphere (40% of all leukemias over the age 65 years) • Median age of presentation is between 65 and 70 years, but 20-30% of patients is under the age of 55 years • 20-30 times commoner in Europe, North American white and black populations than in India, China or Japan • Male/female ratio is appr. 2:1
Chronic lymphocytic leukemia (B-cell CLL)-diagnosis • Lymphocytes > 5 x 109/L; ≥ 1 B-cell marker (CD19, CD20, CD23) + CD5 (without other pan-T cell markers), B-cell is monoclonal (expression of either κ or λ, low density of surface immunoglobulin sIg • Atypical cells (e.g. prolymphocytes) < 55% • Duration of lymphocytosis – none required • Bone marrow lymphocytes ≥ 30%
Chronic lymphocytic leukemia (B-cell CLL) – Rai staging system
B-CLL – indications for treatment • Progressive marrow failure-the development or worsening of anaemia and/or thrombocytopenia • Massive (>10cm) or progressive lymphadenopathy • Massive (>6cm) or progressive splenomegaly • Progressive lymphocytosis: • >50% increase over 2 months • Lymphocyte doubling time (LDT)<6 months • Systemic symptoms • Autoimmune cytopenias (AIHA, ITP)
Management of B-CLL • Patient-related factors (age, PS, co-morbid conditions, patient wishes) • Disease-related factors (the severity of symptoms, adverse prognostic factors) • Treatment-related factors (the degree and duration of response to prior treatments, contra-indications to, side-effects from)
Treatment strategy for B-CLL • Early stage CLL • „watchfull waiting” • „Treatment of early stage with chlorambucil is not indicated” (grade A recomendation, level Ia evidence) • Advanced or progressive disease • Alkylating agents (chlorambucil +/-prednison, COP, CHOP) • Purine analogues (fludarabine, cladribine – alone or in combinations with cyclophosphamide, mitoxantrone) • Monoclonal antibodies (alemtuzumab, rituximab – as a second line treatment) • Transplantation in CLL: autologous transplantation; allogeneic transplantation with low intensity conditioning regimens (RIC-alloTx)
Lymphomatous transformation in CLL • 5-10% of patients with CLL develop more aggressive form of lymphoma - Richter’s transformation of CLL (Richter, 1928) • No standard therapy can be recommended for Richter’s syndrome (CHOP, experimental therapy with monoclonal antibodies, cisplatin/fludarabine based chemotherapy is used)
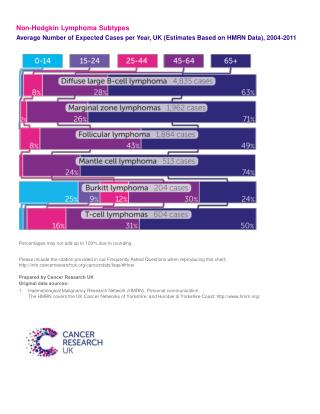
Diffuse large B-cell lymphoma (DLBCL) • The most frequent type of non-Hodgkin’s lymphoma • An aggressive disease if untreated • Quite responsive to chemotherapy (~ 50% of pts may be cured)
Ann Arbor staging system(for non-Hodgkin’s lymphoma and for Hodgkin’s disease)
Ann Arbor staging system(for non-Hodgkin’s lymphoma and for Hodgkin’s disease) cont.
Ann Arbor staging (cont.) • „B” symptoms: fever, night sweats or unexplained loss of 10% or more body weight in the 6 months preceding diagnosis • „A” – absence of these symptoms • „E” – involvement of an extralymphatic site • „S” – splenic involvement
IPI for DLBCL (and aggressive non-Hodgkin’s lymphomas) • Age (<60 vs ≥60) • Tumor stage (I-II vs III-IV) • The number of extranodal sites (≤1 vs >1) • PS (0-1 vs ≥2) • LDH level (normal vs elevated)
IPI for DLBCL (and aggressive non-Hodgkin’s lymphomas) RISK: • Low: 0-1 risk factors • Low-intermediate: 2 risk factors • High-intermediate: 3 risk factors • High: 4-5 risk factors
DLBCL - treatment • Always chemotherapy (CHOP, other regimens) • Chemoimmunotherapy (CHOP+rituximab) • High-dose chemotherapy with autologous-SCT
Follicular lymphoma (FL) • Common in the Western Hemisphere • FL cells closely mimic the cells of the normal germinal center of the lymphoid follicle • Indolent – fewer mitotic figures and less cell turnover than its benign counterpart follicular hyperplasia • Most cases t(14;18), which juxtaposes the bcl-2 gene to Ig Heavy-chain gene
FL – International Prognostic Index (FLIPI) • Age (>60 years vs ≤ 60 years) • Ann Arbor stage (III-IV vs I-II) • Hb level (<12 g/dL vs ≥12 g/dL) • Number of nodal areas (>4 vs ≤4) • Serum LDH level (above normal vs normal or below) • Low risk (0-1 adverse factor, 36% pts) • Intermediate risk (2 factors, 37%) • Poor risk (≥3 factors, 27% pts)
FL - treatment • Chemotherapy (COP, CHOP, others) • Rituximab (monoclonal antibody anti-CD20) alone or in combination with chemotherapy (COP-R, CHOP-R) • SCT for FL (autologous-SCT mostly; allogeneic-SCT mortality 30%) • Radioimmunotherapy (combines the antibody- and complement-dependent cytotoxicity of standard monoclonal antibodies with free radical-mediated apoptosis induced by the radioactive isotope): • 131-Iodine Tositumomab (Bexxar) • 90-Yttrium Ibritumomab Tiuxetan (Zevalin) • New agents (galiximab = anti-CD80, zanolimumab = anti-epitope of CD20, temsirolimus, bortezomib=Velcade)
Cutaneous T-cell Lymphoma (CTCL) • Non-Hodgkin’s lymphoma • Spektrum of disesases composed of malignant clonal helper T lymphocytes of CD4 phenotype • Median pts’ age is 50-55 years • Male to female ratio is 2:1 • Unpredictable course
Cutaneous T-cell Lymphoma (CTCL) • Mycosis fungoides (patches, infiltrated plaques, tumors) • Sezary syndrome (the leukemic variant of CTCL): generalized erythroderma, leukemia and lymphadenopathy; malignant T cells with hyperconvoluted cerebriform nuclei circulate in the blood (Sezary cells)
Cutaneous T-cell Lymphoma (CTCL) - diagnosis • characteristic clinical manifestations • routine histology • immunophenotyping, flow cytometry, T-cell receptor gene rearrangement